Gas gangrene
Topic: Medicine
 From HandWiki - Reading time: 10 min
From HandWiki - Reading time: 10 min
This article needs more medical references for verification or relies too heavily on primary sources. (August 2025) |
| Gas gangrene | |
|---|---|
| Other names | Myonecrosis,[clarification needed] clostridial myonecrosis |
 | |
| Photograph before right leg amputation (hemipelvectomy) of a patient with gas gangrene. The right thigh is edematous (swollen) and discoloured with necrotic bullae (large blisters). Crepitation is detected on deep palpation. At this juncture, the patient is in shock, and died less than eight hours later. | |
| Specialty | Infectious disease |
| Differential diagnosis | Various bacterial infections.[1] |
| Prevention | Proper wound care.[2] |
| Treatment | Hyperbaric medicine, Debridement, and/or excision, with amputation. |
| Prognosis | 5%-30% mortality rate (treated)[3] 100% mortality rate (untreated)[3] |
| Frequency | 1,000 cases (yearly) (USA) |
Gas gangrene (also known as clostridial myonecrosis)[4] is a bacterial infection that produces tissue gas in gangrene. This deadly form of gangrene usually is caused by Clostridium perfringens bacteria. About 1,000 cases of gas gangrene are reported yearly in the United States.[5]
Myonecrosis is a condition of necrotic damage, specific to muscle tissue. It is often seen in infections with C. perfringens or any of myriad soil-borne anaerobic bacteria. Bacteria cause myonecrosis by specific exotoxins. These microorganisms are opportunistic and, in general, enter the body through significant skin breakage. Gangrenous infection by soil-borne bacteria was common in the combat injuries of soldiers well into the 20th century, because of non-sterile field surgery and the basic nature of care for severe projectile wounds.[2]
Other causes of myonecrosis include envenomation by snakes of the genus Bothrops (family Viperidae), ischemic necrosis, caused by vascular blockage (e.g., diabetes type II), tumours that block or hoard blood supply, and disseminated intravascular coagulation or other thromboses.
Presentation

(a) Macroscopic picture of the edematous intestinal wall with multiple submucosal and subserosal cysts
(b) Histological picture of the intestinal mucosa with nonreactive necrosis
(c) Gram stain of cysts with large, rod-shaped bacteria
(d) Electron microscopic picture of a bacterium found in a submucosal cyst

Symptoms
A multitude of symptoms is associated with gas gangrene. Distinctively, black lesions on the skin appear in a bubble form which allows visualization of gas-producing bacteria. Symptoms include:[6]
- Skin discoloration
- "Foul, sweet" smelling discharge from lesions formed on skin
- Distinctive black, bubble lesions on skin
- Necrosis
- Fever
- Pain at site of surgery or trauma
- Lightheadedness
- Rapid heart rate
- Numbness of affected site
- Blisters
- Air in subcutaneous tissues (crepitus)
- Swelling
- Jaundice
Etiology
Clostridium species produce more toxins and exhibit higher degrees of virulence than any other bacterial taxon.[7] Clostridium infections are usually opportunistic, and occur in individuals with serious preexisting medical conditions. However, Clostridium infections are also known to occur in healthy individuals. Four species of Clostridium (Clostridium botulinum, Clostridium perfringens, Clostridium tetani, and Clostridium sordelli) are responsible for most human infections. Since Clostridium is an obligate anaerobe taxon, the bacterium infects hypoxic tissues, which have become anaerobic due to restricted blood flow, degradation of blood vessels, or atherosclerosis. Immunocompromised individuals exhibit higher susceptibility for infection and higher mortality rates.
Virulence factors
The key Clostridium septicum virulence factor is a pore-forming toxin called alpha-toxin, though it is unrelated to the Clostridium perfringens alpha-toxin.
Clostridium sordellii can also produce two major toxins: all known virulent strains produce the essential virulence factor lethal toxin (TcsL), and a number also produce haemorrhagic toxin (TcsH). TcsL and TcsH are both members of the large clostridial cytotoxin (LCC) family.
- Clostridium perfringens alpha toxin (α-toxin)
C. perfringens alpha toxin is widely associated with gas gangrene as it is its main virulence factor whilst invading its host. Alpha-toxin causes excessive platelet aggregation which blocks blood vessels and deprives the vital organs of oxygen supply. This creates an acidic, oxygen-deficient environment that helps bacteria grow. When alpha-toxin is absorbed by soft tissues, it can also inhibit the migration of white blood cells from blood vessels into the soft tissue, thus impairing phagocyte function. As the surrounding circulatory system collapses, neutrophils and monocytes, eosinophils and basophils cannot reach target areas of infection.
- Theta toxin (Θ-toxin)
Theta toxin is also employed by C. perfringens as a virulence factor. Theta toxin also promotes vascular degradation as does its counterpart alpha toxin. A platelet-activation factor is employed which triggers an acute inflammatory response in nearby tissues.[8] This inflammatory response leads to constriction of surrounding arteries and promotes an anaerobic environment for C. perfringens growth and pathophysiology.
- Beta toxin (β-toxin)
Beta toxin is an integral virulence factor in promoting enterocolitis and enterotoxemia.[9] This toxin uses pores in the cellular biolipid membrane to import a pathogenic factor into organisms.
Pathophysiology
Gas gangrene is caused by exotoxin-producing Clostridium species (most often C. perfringens, and C. novyi,[10][11] but less commonly C. septicum[12] or C. ramnosum),[13] which are mostly found in soil, but also found as normal gut flora, and other anaerobes (e.g., Bacteroides and anaerobic streptococci). Bacterium of the Clostridial species produce two toxins: alpha and theta toxins, which cause necrotizing damage to tissues.[14]
Other organisms may occasionally cause gas gangrene (for example, Klebsiella pneumoniae in the context of diabetes).[15]
A gas composition of 5.9% hydrogen, 3.4% carbon dioxide, 74.5% nitrogen, and 16.1% oxygen was reported in one clinical case.[16]
It is often difficult to identify the extent of muscle damage, as C. perfringens may be at work in deeper fascial layers below the skin. Unlike other anaerobic infections, discharge in these infections is often not purulent (filled with pus). Instead, the discharge is often described as "sweetly putrid" or "dishwater pus" because it is much thinner than normal pus. This is due to the lysis of neutrophils, a type of white blood cell, caused by the lecithinases and other toxins released by Clostridium species.[1]
Soil-borne anaerobes are particularly well-adapted to surviving harsh conditions. Often, a scarcity of nutrition and competition for resources from numerous other species occurs. Changes in pH and temperature are often significant, also. Bacteria often possess the ability to create exotoxins to assist them in competing with other microbes in their natural environments. When such bacteria are able to enter a living host, they encounter a vast supply of nutrients, warm conditions, and an abundance of water. This enables the microbes to rapidly proliferate, far in excess of the immune system's capability to defend, as prokaryotic bacteria possess a far greater capacity for multiplication than the host's immune system. The combination of bacterial load and ability to multiply is the basis for the microbes' ability to cause massive infection. Alongside such rapid proliferation is a corresponding mass-production of exotoxin that causes severe damage to local tissue in the host. One such exotoxin is alpha toxin, which is produced by C. perfringens and is the key virulence factor in its pathogenesis.[17]
Diagnosis
Various diagnostic methods can be employed in the diagnosis of Gas gangrene. Due to low incidence of myonecrosis it is an easy-to-overlook diagnosis.[18] As bacterial infections mostly exhibit the same symptoms, early diagnosis of gas gangrene rarely occurs. The ambiguous symptoms only contribute to a poorer prognosis. Diagnostic methods include:[1]
- Biopsy of affected tissue
- Cultures of fluids from inflicted area
- Magnetic resonance imaging to visualize necrotized subcutaneous tissues
- X-rays for air pockets in affected tissues
- Microscopy identification of strain of bacteria sampled from fluids of inflicted area
- Gram stain
Treatment
Treatment is usually debridement and excision, with amputation necessary in many cases. Water-soluble antibiotics (such as penicillin) alone are not effective because they do not penetrate ischaemic muscles sufficiently to be effective. Penicillin is effective against C. perfringens. When gas gangrene occurs in such regions as the abdominal cavity, the patient can be treated in a hyperbaric chamber, which contains a pressurized oxygen-rich atmosphere. The oxygen saturates the infected tissues and thereby prevents the growth of the obligately anaerobic clostridia.[19] The growth of C. perfringens is inhibited when the availability of oxygen is equivalent to a partial pressure of around 9–10 kPa (compare to 4–5 kPa in venous blood under normal conditions, with 11–13 kPa in arteries and 21 kPa in air at sea level), so if the treatment is started early, this condition can mostly be cured.[20]
Prognosis
Following resolution of myonecrosis, patients will often require further care following the deleterious effects caused by the infection. Skin grafts are often required following removal of necrotic tissues. Former patients will still require hyperbaric oxygen therapy to prevent a recurring infection.[21]
Epidemiology
Clostridium species are found in abundance in soil, especially soil used for animal husbandry.[7] In medical facilities, it thrives when unhygienic circumstances prevail. In the United States, the incidence of myonecrosis is only about 1,000 cases per year.[3]
During World War I and World War II, Clostridial myonecrosis was found in 5% of wounds, but with improvement in wound care, antisepsis and the use of antibiotics, the incidence had fallen to 0.1% of war-related wound infections by the Vietnam War.[3]
Gas gangrene reappeared during the Russo-Ukraine War.[22]
Additional images
-
 Hemipelvectomy for gas gangrene
Hemipelvectomy for gas gangrene -
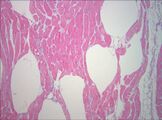 Muscle biopsy examined under the microscope (haematoxylin-eosin stain, zoom 100×): the large white areas between the muscle fibers are due to gas formation.
Muscle biopsy examined under the microscope (haematoxylin-eosin stain, zoom 100×): the large white areas between the muscle fibers are due to gas formation. -
 Gram stain of a muscle biopsy showing Gram-positive, rod-shaped, anaerobic, spore-forming bacteria in the infected muscle tissue: The result is highly compatible with an infection with C. perfringens.
Gram stain of a muscle biopsy showing Gram-positive, rod-shaped, anaerobic, spore-forming bacteria in the infected muscle tissue: The result is highly compatible with an infection with C. perfringens. -
 Gas gangrene of the shoulder.
Gas gangrene of the shoulder.




See also
- Blackleg (a similar disease in livestock)
- List of cutaneous conditions
References
- ↑ 1.0 1.1 1.2 "Gas Gangrene". https://www.lecturio.com/concepts/gas-gangrene/.
- ↑ 2.0 2.1 "La gangrène gazeuse: une affection militaire?" (in fr). Acta Chir. Belg. 86 (2): 63–71. 1986. PMID 3716723.
- ↑ 3.0 3.1 3.2 3.3 Buboltz, J. B.; Murphy-Lavoie, H. M. (2021). "Gas Gangrene". StatPearls. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK537030/.
- ↑ James, William D. et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. p. 269. ISBN 978-0-7216-2921-6. https://archive.org/details/andrewsdiseasess00mdwi_659.
- ↑ Jerrold B. Leikin; Frank P. Paloucek, eds. (2008), Poisoning and Toxicology Handbook (4th ed.), Informa, pp. 892–893, ISBN 978-1-4200-4479-9
- ↑ "Gas gangrene" (in en). https://www.amboss.com/us/knowledge/Gas_gangrene.
- ↑ 7.0 7.1 Bryant, Amy E.; Stevens, Dennis L.. "179: Gas Gangrene and Other Clostridial Infections". Harrison's Principles of Internal Medicine (19th ed.). https://accessmedicine.mhmedical.com/content.aspx?bookid=1130§ionid=79735535. Retrieved 1 May 2020.
- ↑ "Role of theta toxin, a sulfhydryl-activated cytolysin, in the pathogenesis of clostridial gas gangrene". Clin. Infect. Dis. 16 (Suppl 4): S195–S199. June 1993. doi:10.1093/clinids/16.supplement_4.s195. PMID 8324118.
- ↑ Masahiro, Nagahama; Sadayuki, Ochi; Masataka, Oda; Kazuaki, Miyamoto; Keiko, Kobayashi (February 3, 2015). "Recent Insights into Clostridium perfringens Beta-Toxin". Toxins (Basel) 7 (2): 396–406. doi:10.3390/toxins7020396. PMID 25654787.
- ↑ Hatheway CL (January 1990). "Toxigenic clostridia". Clin. Microbiol. Rev. 3 (1): 66–98. doi:10.1128/CMR.3.1.66. PMID 2404569.
- ↑ Busch, Christian; Schömig, Kathrin; Hofmann, Fred; Aktories, Klaus (November 2000). "Characterization of the Catalytic Domain of Clostridium novyi Alpha-Toxin". Infection and Immunity 68 (11): 6378–6383. doi:10.1128/iai.68.11.6378-6383.2000. PMID 11035748.
- ↑ "Clostridium septicum infections in children". Pediatr Infect Dis J 11 (7): 569–75. 1992. doi:10.1097/00006454-199207000-00011. PMID 1528648.
- ↑ "Gas gangrene in an immunocompromised girl due to a Clostridium ramosum infection". Clin. Infect. Dis. 28 (4): 923–4. April 1999. doi:10.1086/517249. PMID 10825071.
- ↑ Buboltz, Jerome B.; Murphy-Lavoie, Heather M. (October 13, 2019). Gas Gangrene. https://www.ncbi.nlm.nih.gov/books/NBK537030/. Retrieved 1 May 2020.
- ↑ "Shortness of breath, fever—and pain in both legs". Lancet 372 (9648): 1518. 2008. doi:10.1016/S0140-6736(08)61621-9. PMID 18970978.
- ↑ ^ "Gas composition in Clostridium septicum gas gangrene". J Formos Med Assoc 94 (12): 757–9. 1995. PMID 8541740.
- ↑ "Virulence studies on chromosomal alpha-toxin and theta-toxin mutants constructed by allelic exchange provide genetic evidence for the essential role of alpha-toxin in Clostridium perfringens-mediated gas gangrene". Mol. Microbiol. 15 (2): 191–202. January 1995. doi:10.1111/j.1365-2958.1995.tb02234.x. PMID 7746141.
- ↑ Brucato, Maryellen P.; Patel, Krupa; Mgbako, Obinna (2014). "Diagnosis of gas gangrene: does a discrepancy exist between the published data and practice". The Journal of Foot and Ankle Surgery 53 (2): 137–140. doi:10.1053/j.jfas.2013.10.009. ISSN 1542-2224. PMID 24345706.
- ↑ Gerard J. Tortora; Berdell R. Funke; Christine L. Case (2010), Microbiology: An Introduction (10th ed.), Benjamin Cummings, p. 646, ISBN 978-0-321-55007-1
- ↑ Guyton and Hall. Textbook of Medical Physiology, 12th edition, chapter 44, "Physiological issues in deep-sea diving and other high-pressure conditions"
- ↑ "Gas Gangrene". StatPearls [Internet] (Treasure Island (FL): StatPearls Publishing). October 13, 2019. PMID 30725715. https://www.ncbi.nlm.nih.gov/books/NBK537030/. Retrieved 1 May 2020.
- ↑ https://www.telegraph.co.uk/global-health/terror-and-security/gas-gangrene-ukraine-war-russia-trenches-europe/
| Classification | |
|---|---|
| External resources |
Template:Bacterial cutaneous infections
 |  |
 EncycloReader
is supported by the
EncycloReader
is supported by the