Categories
Bosentan
 From Wikidoc - Reading time: 28 min
From Wikidoc - Reading time: 28 min
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Gerald Chi
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
WARNING: RISKS OF HEPATOTOXICITY and TERATOGENICITY
See full prescribing information for complete Boxed Warning.
* Because of the risks of hepatotoxicity and birth defects, Tracleer is available only through a restricted program called the Tracleer Access Program (T.A.P.). T.A.P. is a component of the Tracleer Risk Evaluation and Mitigation Strategy (REMS). Under the Tracleer REMS, prescribers, patients, and pharmacies must enroll in the program.
Hepatotoxicity:
Teratogenicity:
|
Overview
Bosentan is an endothelin receptor antagonist that is FDA approved for the {{{indicationType}}} of pulmonary arterial hypertension. There is a Black Box Warning for this drug as shown here. Common adverse reactions include edema, hypotension, palpitations, flushing, and headache.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Pulmonary Arterial Hypertension
- Tracleer® is indicated for the treatment of pulmonary arterial hypertension (PAH) (WHO Group 1) to improve exercise ability and to decrease clinical worsening. Studies establishing effectiveness included predominantly patients with NYHA Functional Class II-IV symptoms and etiologies of idiopathic or heritable PAH (60%), PAH associated with connective tissue diseases (21%), and PAH associated with congenital heart disease with left-to-right shunts (18%).
- Patients with WHO Class II symptoms showed reduction in the rate of clinical deterioration and a trend for improvement in walk distance. Physicians should consider whether these benefits are sufficient to offset the risk of hepatotoxicity in WHO Class II patients, which may preclude future use as their disease progresses.
- Healthcare professionals who prescribe Tracleer must enroll in the Tracleer Access Program (T.A.P.) and must comply with the required monitoring to minimize the risks associated with Tracleer.
- Dosing Information
- Initiate treatment at 62.5 mg twice daily for 4 weeks and then increase to the maintenance dose of 125 mg twice daily. Doses above 125 mg twice daily did not appear to confer additional benefit sufficient to offset the increased risk of hepatotoxicity.
- Tracleer should be administered in the morning and evening with or without food.
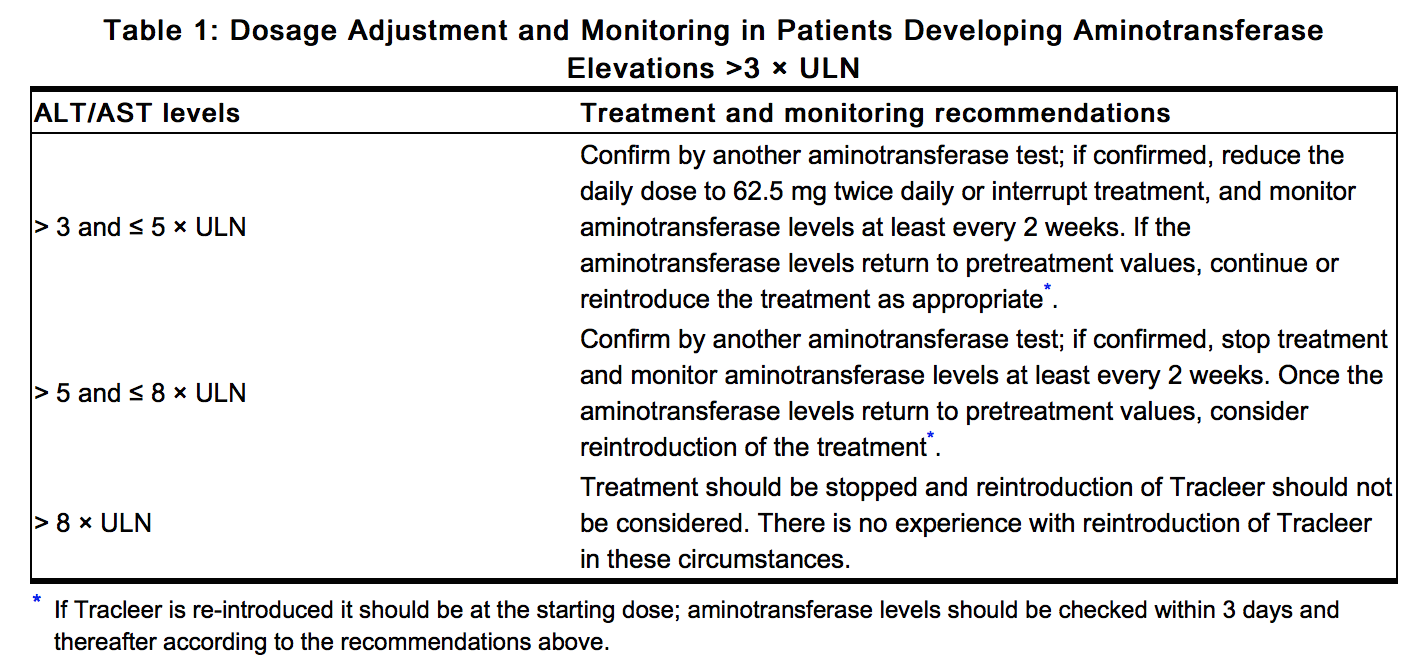
Dosage Adjustments for Patients Developing Aminotransferase Elevations
- Measure liver aminotransferase levels prior to initiation of treatment and then monthly. If aminotransferase levels increase, revise the monitoring and treatment plan. The table below summarizes the dosage adjustment and monitoring recommendations for patients who develop aminotransferase elevations >3 × ULN during therapy with Tracleer. Discontinue Tracleer if liver aminotransferase elevations are accompanied by clinical symptoms of hepatotoxicity (such as nausea, vomiting, fever, abdominal pain, jaundice, or unusual lethargy or fatigue) or increases in bilirubin ≥ 2 × ULN. There is no experience with the reintroduction of Tracleer in these circumstances. Information.
This image is provided by the National Library of Medicine.

Patients with Low Body Weight
- In patients with a body weight below 40 kg but who are over 12 years of age, the recommended initial and maintenance dose is 62.5 mg twice daily. There is limited information about the safety and efficacy of Tracleer in children between the ages of 12 and 18 years.
Use with Ritonavir
- Coadministration of Tracleer in Patients on Ritonavir
- In patients who have been receiving ritonavir for at least 10 days, start Tracleer at 62.5 mg once daily or every other day based upon individual tolerability.
- Coadministration of Ritonavir in Patients on Tracleer
Use in Patients with Pre-existing Hepatic Impairment
- Tracleer should generally be avoided in patients with moderate or severe liver impairment. Initiation of Tracleer should generally be avoided in patients with elevated aminotransferases >3 × ULN. No dose adjustment is required in patients with mildly impaired liver function.
Treatment Discontinuation
- There is limited experience with abrupt discontinuation of Tracleer. No evidence for acute rebound has been observed. Nevertheless, to avoid the potential for clinical deterioration, gradual dose reduction (62.5 mg twice daily for 3 to 7 days) should be considered.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Bosentan in adult patients.
Non–Guideline-Supported Use
Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
- Dosing Information
- 62.5 mg orally twice daily for 4 weeks, followed by 125 mg twice daily or 62.5 mg twice daily in patients weighing less than 40 kilograms.[1]
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
- Safety and efficacy in pediatric patients have not been established.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Bosentan in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Bosentan in pediatric patients.
Contraindications
- Pregnancy
- Use of Tracleer is contraindicated in females who are or may become pregnant. To prevent pregnancy, females of childbearing potential must use two reliable forms of contraception during treatment and for one month after stopping Tracleer.
- Use with Cyclosporine A
- Coadministration of cyclosporine A and bosentan resulted in markedly increased plasma concentrations of bosentan. Therefore, concomitant use of Tracleer and cyclosporine A is contraindicated.
- Use with Glyburide
- Hypersensitivity
- Tracleer is contraindicated in patients who are hypersensitive to bosentan or any component of the product. Observed reactions include rash and angioedema.
Warnings
|
WARNING: RISKS OF HEPATOTOXICITY and TERATOGENICITY
See full prescribing information for complete Boxed Warning.
* Because of the risks of hepatotoxicity and birth defects, Tracleer is available only through a restricted program called the Tracleer Access Program (T.A.P.). T.A.P. is a component of the Tracleer Risk Evaluation and Mitigation Strategy (REMS). Under the Tracleer REMS, prescribers, patients, and pharmacies must enroll in the program.
Hepatotoxicity:
Teratogenicity:
|
- Hepatotoxicity
- Elevations in ALT or AST by more than 3 × ULN were observed in 11% of Tracleer-treated patients (n = 658) compared to 2% of placebo-treated patients (n = 280). Three-fold increases were seen in 12% of 95 pulmonary arterial hypertension (PAH) patients on 125 mg twice daily and 14% of 70 PAH patients on 250 mg twice daily. Eight-fold increases were seen in 2% of PAH patients on 125 mg twice daily and 7% of PAH patients on 250 mg twice daily. Bilirubin increases to ≥3 × ULN were associated with aminotransferase increases in 2 of 658 (0.3%) of patients treated with Tracleer. The combination of hepatocellular injury (increases in aminotransferases of > 3 × ULN) and increases in total bilirubin (≥ 2× ULN) is a marker for potential serious hepatotoxicity.
- Elevations of AST or ALT associated with Tracleer are dose-dependent, occur both early and late in treatment, usually progress slowly, are typically asymptomatic, and usually have been reversible after treatment interruption or cessation. Aminotransferase elevations also may reverse spontaneously while continuing treatment with Tracleer.
- Liver aminotransferase levels must be measured prior to initiation of treatment and then monthly and therapy adjusted accordingly. Discontinue Tracleer if liver aminotransferase elevations are accompanied by clinical symptoms of hepatotoxicity (such as nausea, vomiting, fever, abdominal pain, jaundice, or unusual lethargy or fatigue) or increases in bilirubin ≥ 2 × ULN.
- Prescribing and Distribution Program for Tracleer
- Because of the risks of hepatotoxicity and birth defects, Tracleer is available only through a restricted program called the Tracleer Access Program (T.A.P.) As a component of the Tracleer REMS, prescribers, patients, and pharmacies must enroll in the program.
- Required components of the Tracleer REMS are:
- Healthcare professionals who prescribe Tracleer must review the prescriber educational materials, enroll in T.A.P. and comply with its requirements.
- Healthcare professionals must (1) review serum aminotransferases (ALT/AST) and bilirubin, and agree to order and monitor these tests monthly; and (2) for females of childbearing potential, confirm that the patient is not pregnant, and agree to order and monitor pregnancy tests monthly.
- To receive Tracleer, all patients must understand the risks and benefits, complete a patient enrollment form, and be re-enrolled annually by their prescriber.
- Pharmacies that dispense Tracleer must enroll in the program and agree to comply with the T.A.P. requirements.
- Further information about Tracleer and T.A.P. is available at www.tracleerrems.com or 1-866-228-3546.
- Patients with Pre-existing Hepatic Impairment
- Tracleer is not recommended in patients with moderate or severe liver impairment. In addition, initiation of Tracleer should generally be avoided in patients with elevated aminotransferases (> 3 × ULN) prior to drug initiation because monitoring hepatotoxicity in these patients may be more difficult.
- Fluid Retention
- Peripheral edema is a known clinical consequence of PAH and worsening PAH and is also a known effect of Tracleer and other endothelin receptor antagonists. In PAH clinical trials with Tracleer, combined adverse events of fluid retention or edema were reported in 1.7 percent (placebo-corrected) of patients
- In addition, there have been numerous postmarketing reports of fluid retention in patients with pulmonary hypertension occurring within weeks after starting Tracleer. Patients required intervention with a diuretic, fluid management, or hospitalization for decompensating heart failure.
- If clinically significant fluid retention develops, with or without associated weight gain, further evaluation should be undertaken to determine the cause, such as Tracleer or underlying heart failure, and the possible need for treatment or discontinuation of Tracleer.
- Pulmonary Veno-Occlusive Disease
- Should signs of pulmonary edema occur, consider the possibility of associated pulmonary veno-occlusive disease and consider whether Tracleer should be discontinued.
- Decreased Sperm Counts
- Decreased sperm counts have been observed in patients receiving Tracleer. Preclinical data also suggest that Tracleer, like other endothelin receptor antagonists, may have an adverse effect on spermatogenesis.
- Decreases in Hemoglobin and Hematocrit
- Treatment with Tracleer can cause a dose-related decrease in hemoglobin and hematocrit. There have been postmarketing reports of decreases in hemoglobin concentration and hematocrit that have resulted in anemia requiring transfusion. It is recommended that hemoglobin concentrations be checked after 1 and 3 months, and every 3 months thereafter. If a marked decrease in hemoglobin concentration occurs, further evaluation should be undertaken to determine the cause and need for specific treatment.
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
- Safety data on Tracleer were obtained from 13 clinical studies (9 placebo-controlled and 4 open-label) in 870 patients with pulmonary arterial hypertension and other diseases. Doses up to 8 times the currently recommended clinical dose (125 mg twice daily) were administered for a variety of durations. The exposure to Tracleer in these trials ranged from 1 day to 4.1 years (n=94 for 1 year; n=61 for 1.5 years and n=39 for more than 2 years). Exposure of pulmonary arterial hypertension patients (n=328) to Tracleer ranged from 1 day to 1.7 years (n=174 more than 6 months and n=28 more than 12 months).
- Treatment discontinuations due to adverse events other than those related to pulmonary hypertension during the clinical trials in patients with pulmonary arterial hypertension were more frequent on Tracleer (6%; 15/258 patients) than on placebo (3%; 5/172 patients). In this database the only cause of discontinuations > 1% and occurring more often on Tracleer was abnormal liver function.
- The adverse drug events that occurred in ≥3% of the Tracleer-treated patients and were more common on Tracleer in placebo-controlled trials in pulmonary arterial hypertension at doses of 125 or 250 mg twice daily are shown in Table 2:

This image is provided by the National Library of Medicine.

Decreased Sperm Counts
- An open-label, single arm, multicenter, safety study evaluated the effect on testicular function of Tracleer 62.5 mg twice daily for 4 weeks, followed by 125 mg twice daily for 5 months. Twenty-five male patients with WHO functional class III and IV PAH and normal baseline sperm count were enrolled. Twenty-three completed the study and 2 discontinued due to adverse events not related to testicular function. There was a decline in sperm count of at least 50% in 25% of the patients after 3 or 6 months of treatment with Tracleer. Sperm count remained within the normal range in all 22 patients with data after 6 months and no changes in sperm morphology, sperm motility, or hormone levels were observed. One patient developed marked oligospermia at 3 months and the sperm count remained low with 2 follow-up measurements over the subsequent 6 weeks. Tracleer was discontinued and after 2 months the sperm count had returned to baseline levels. Based on these findings and preclinical data from endothelin receptor antagonists, it cannot be excluded that endothelin receptor antagonists such as Tracleer have an adverse effect on spermatogenesis.
Decreases in Hemoglobin and Hematocrit
- Treatment with Tracleer can cause a dose-related decrease in hemoglobin and hematocrit. It is recommended that hemoglobin concentrations be checked after 1 and 3 months, and every 3 months thereafter. If a marked decrease in hemoglobin concentration occurs, further evaluation should be undertaken to determine the cause and need for specific treatment.
- The overall mean decrease in hemoglobin concentration for Tracleer-treated patients was 0.9 g/dL (change to end of treatment). Most of this decrease of hemoglobin concentration was detected during the first few weeks of Tracleer treatment and hemoglobin levels stabilized by 4–12 weeks of Tracleer treatment. In placebo-controlled studies of all uses of Tracleer, marked decreases in hemoglobin (> 15% decrease from baseline resulting in values < 11 g/dL) were observed in 6% of Tracleer-treated patients and 3% of placebo-treated patients. In patients with PAH treated with doses of 125 and 250 mg twice daily, marked decreases in hemoglobin occurred in 3% compared to 1% in placebo-treated patients.
- A decrease in hemoglobin concentration by at least 1 g/dL was observed in 57% of Tracleer-treated patients as compared to 29% of placebo-treated patients. In 80% of those patients whose hemoglobin decreased by at least 1 g/dL, the decrease occurred during the first 6 weeks of Tracleer treatment.
- During the course of treatment the hemoglobin concentration remained within normal limits in 68% of Tracleer-treated patients compared to 76% of placebo patients. The explanation for the change in hemoglobin is not known, but it does not appear to be hemorrhage or hemolysis.
Postmarketing Experience
- There have been several postmarketing reports of angioedema associated with the use of Tracleer. The onset of the reported cases occurred within a range of 8 hours to 21 days after starting therapy. Some patients were treated with an antihistamine and their signs of angioedema resolved without discontinuing Tracleer.
- The following additional adverse reactions have been reported during the postapproval use of Tracleer. Because these adverse reactions are reported from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to Tracleer exposure:
- Unexplained hepatic cirrhosis
- Liver failure
- Hypersensitivity
- Thrombocytopenia
- Rash
- Jaundice
- Anemia requiring transfusion
- Neutropenia and leukopenia
Drug Interactions
Cytochrome P450 Summary
- Bosentan is metabolized by CYP2C9 and CYP3A. Inhibition of these enzymes may increase the plasma concentration of bosentan (see ketoconazole). Concomitant administration of both a CYP2C9 inhibitor (such as fluconazole or amiodarone) and a strong CYP3A inhibitor (e.g., ketoconazole, itraconazole) or a moderate CYP3A inhibitor (e.g., amprenavir, erythromycin, fluconazole, diltiazem) with Tracleer will likely lead to large increases in plasma concentrations of bosentan. Coadministration of such combinations of a CYP2C9 inhibitor plus a strong or moderate CYP3A inhibitor with Tracleer is not recommended.
- Bosentan is an inducer of CYP3A and CYP2C9. Consequently plasma concentrations of drugs metabolized by these two isozymes will be decreased when Tracleer is coadministered. Bosentan had no relevant inhibitory effect on any CYP isozyme in vitro (CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP3A). Consequently, Tracleer is not expected to increase the plasma concentrations of drugs metabolized by these enzymes.
Hormonal Contraceptives
- Hormonal contraceptives, including oral, injectable, transdermal, and implantable forms, may not be reliable when Tracleer is coadministered. Females should practice additional methods of contraception and not rely on hormonal contraception alone when taking Tracleer.
- An interaction study demonstrated that coadministration of bosentan and a combination oral hormonal contraceptive produced average decreases of norethindrone and ethinyl estradiol levels of 14% and 31%, respectively. However, decreases in exposure were as much as 56% and 66%, respectively, in individual subjects.
Cyclosporine A
- The concomitant administration of Tracleer and cyclosporine A is contraindicated.
- During the first day of concomitant administration, trough concentrations of bosentan were increased by about 30-fold. The mechanism of this interaction is most likely inhibition of transport protein-mediated uptake of bosentan into hepatocytes by cyclosporine. Steady-state bosentan plasma concentrations were 3- to 4-fold higher than in the absence of cyclosporine A. Coadministration of bosentan decreased the plasma concentrations of cyclosporine A (a CYP3A substrate) by approximately 50%.
Glyburide
- An increased risk of elevated liver aminotransferases was observed in patients receiving concomitant therapy with glyburide. Therefore, the concomitant administration of Tracleer and glyburide is contraindicated, and alternative hypoglycemic agents should be considered.
- Coadministration of bosentan decreased the plasma concentrations of glyburide by approximately 40%. The plasma concentrations of bosentan were also decreased by approximately 30%. Tracleer is also expected to reduce plasma concentrations of other oral hypoglycemic agents that are predominantly metabolized by CYP2C9 or CYP3A. The possibility of worsened glucose control in patients using these agents should be considered.
Lopinavir/Ritonavir or Other Ritonavir-containing HIV Regimens
- In vitro data indicate that bosentan is a substrate of the Organic Anion Transport Protein (OATP), CYP3A and CYP2C9. Ritonavir inhibits OATP and inhibits and induces CYP3A. However, the impact of ritonavir on the pharmacokinetics of bosentan may largely result from its effect on OATP.
- In normal volunteers, coadministration of Tracleer 125 mg twice daily and lopinavir/ritonavir 400/100 mg twice daily increased the trough concentrations of bosentan on Days 4 and 10 approximately 48-fold and 5-fold, respectively, compared with those measured after Tracleer administered alone. Therefore, adjust the dose of Tracleer when initiating lopinavir/ritonavir.
- Coadministration of bosentan 125 mg twice daily had no substantial impact on the pharmacokinetics of lopinavir/ritonavir 400/100 mg twice daily.
Simvastatin and Other Statins
- Coadministration of bosentan decreased the plasma concentrations of simvastatin (a CYP3A substrate), and its active β-hydroxy acid metabolite, by approximately 50%. The plasma concentrations of bosentan were not affected. Tracleer is also expected to reduce plasma concentrations of other statins that are significantly metabolized by CYP3A, such as lovastatin and atorvastatin. The possibility of reduced statin efficacy should be considered. Patients using CYP3A-metabolized statins should have cholesterol levels monitored after Tracleer is initiated to see whether the statin dose needs adjustment.
Rifampin
- Coadministration of bosentan and rifampin in normal volunteers resulted in a mean 6-fold increase in bosentan trough levels after the first concomitant dose (likely due to inhibition of OATP by rifampin), but about a 60% decrease in bosentan levels at steady-state. The effect of Tracleer on rifampin levels has not been assessed. When consideration of the potential benefits, and known and unknown risks leads to concomitant use, measure serum aminotransferases weekly for the first 4 weeks before reverting to normal monitoring.
Tacrolimus
- Coadministration of tacrolimus and Tracleer has not been studied in humans. Coadministration of tacrolimus and bosentan resulted in markedly increased plasma concentrations of bosentan in animals. Caution should be exercised if tacrolimus and Tracleer are used together.
Ketoconazole
- Coadministration of bosentan 125 mg twice daily and ketoconazole, a potent CYP3A inhibitor, increased the plasma concentrations of bosentan by approximately 2-fold in normal volunteers. No dose adjustment of Tracleer is necessary, but increased effects of Tracleer should be considered.
Warfarin
- Coadministration of bosentan 500 mg twice daily for 6 days in normal volunteers decreased the plasma concentrations of both S-warfarin (a CYP2C9 substrate) and R-warfarin (a CYP3A substrate) by 29 and 38%, respectively. Clinical experience with concomitant administration of Tracleer and warfarin in patients with pulmonary arterial hypertension did not show clinically relevant changes in INR or warfarin dose (baseline vs. end of the clinical studies), and the need to change the warfarin dose during the trials due to changes in INR or due to adverse events was similar among Tracleer- and placebo-treated patients.
Digoxin, Nimodipine, and Losartan
- Bosentan has no significant pharmacokinetic interactions with digoxin and nimodipine, and losartan has no significant effect on plasma levels of bosentan.
Sildenafil
- In normal volunteers, coadministration of multiple doses of 125 mg twice daily bosentan and 80 mg three times daily sildenafil resulted in a reduction of sildenafil plasma concentrations by 63% and increased bosentan plasma concentrations by 50%. The changes in plasma concentrations were not considered clinically relevant and dose adjustments are not necessary. This recommendation holds true when sildenafil is used for the treatment of pulmonary arterial hypertension or erectile dysfunction.
Iloprost
- In a small, randomized, double-blind, placebo-controlled study, 34 patients treated with bosentan 125 mg twice daily for at least 16 weeks tolerated the addition of inhaled iloprost (up to 5 mcg 6 to 9 times per day during waking hours). The mean daily inhaled dose was 27 mcg and the mean number of inhalations per day was 5.6.
Use in Specific Populations
Pregnancy
- Pregnancy Category X
- Use of Tracleer is contraindicated in females who are or may become pregnant. While there are no adequate and well-controlled studies in pregnant females, animal studies show that Tracleer is likely to cause major birth defects when administered during pregnancy. Bosentan caused teratogenic effects in animals including malformations of the head, mouth, face, and large blood vessels. If Tracleer is used during pregnancy or if a patient becomes pregnant while taking Tracleer, the patient should be apprised of the potential hazard to the fetus.
- Females of childbearing potential should have a negative pregnancy test before starting treatment with Tracleer. The prescriber should not dispense a prescription for Tracleer without documenting a negative urine or serum pregnancy test performed during the first 5 days of a normal menstrual period and at least 11 days after the last unprotected act of sexual intercourse. Follow-up urine or serum pregnancy tests should be obtained monthly in females of childbearing potential taking Tracleer. The patient should contact her physician immediately for pregnancy testing if onset of menses is delayed or pregnancy is suspected. If the pregnancy test is positive, the physician and patient must discuss the risks to her, the pregnancy, and the fetus.
- Drug interaction studies show that bosentan reduces serum levels of the estrogen and progestin in oral contraceptives. Based on these findings, hormonal contraceptives (including oral, injectable, transdermal, and implantable contraceptives) may be less effective for preventing pregnancy in patients using Tracleer and should not be used as a patient's only contraceptive method. Females of childbearing potential using Tracleer must use two reliable forms of contraception unless she has a tubal sterilization or has a Copper T 380A IUD or LNg 20 IUS. In these cases, no additional contraception is needed. Contraception should be continued until one month after completing Tracleer therapy. Females of childbearing potential using Tracleer should seek contraception counseling from a gynecologist or other expert as needed.
- Bosentan was teratogenic in rats given oral doses two times the maximum recommended human dose [MRHD] (on a mg/ m2 basis). In an embryo-fetal toxicity study in rats, bosentan showed dose-dependent teratogenic effects, including malformations of the head, mouth, face and large blood vessels. Bosentan increased stillbirths and pup mortality at oral doses 2 and 10 times the MRHD (on a mg/m2 basis). Although birth defects were not observed in rabbits given oral doses of up to the equivalent of 10.5 g/day in a 70 kg person, plasma concentrations of bosentan in rabbits were lower than those reached in the rat. The similarity of malformations induced by bosentan and those observed in endothelin-1 knockout mice and in animals treated with other endothelin receptor antagonists indicates that teratogenicity is a class effect of these drugs.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Bosentan in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Bosentan during labor and delivery.
Nursing Mothers
- It is not known whether bosentan is excreted into human milk. Because many drugs are excreted in human milk, and because of the potential for serious adverse reactions in nursing infants from bosentan, a decision should be made to discontinue nursing or to discontinue Tracleer, taking into account the importance of Tracleer to the mother.
Pediatric Use
- Safety and efficacy in pediatric patients have not been established.
Geriatic Use
- Clinical studies of Tracleer did not include sufficient numbers of subjects aged 65 and older to determine whether they respond differently from younger subjects.
Gender
There is no FDA guidance on the use of Bosentan with respect to specific gender populations.
Race
There is no FDA guidance on the use of Bosentan with respect to specific racial populations.
Renal Impairment
- The effect of renal impairment on the pharmacokinetics of bosentan is small and does not require dosing adjustment.
Hepatic Impairment
- Because there is in vitro and in vivo evidence that the main route of excretion of bosentan is biliary, liver impairment could be expected to increase exposure (Cmax and AUC) of bosentan. The pharmacokinetics of Tracleer has not been evaluated in patients with severe liver impairment (Child-Pugh Class C). In patients with moderate hepatic impairment (Child-Pugh Class B), the systemic exposures to bosentan and its active metabolite increased significantly. Tracleer should generally be avoided in patients with moderate or severe liver impairment. Pharmacokinetics of bosentan was not altered in patients with mild impairment of hepatic function (Child-Pugh Class A).
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Bosentan in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Bosentan in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
- Reduce the dose and closely monitor patients developing aminotransferase elevations >3 × ULN.
- Monitor hemoglobin levels after 1 and 3 months of treatment, then every 3 months thereafter.
- Rifampin alters bosentan exposure. Monitor hepatic function weekly for 4 weeks, followed by normal monitoring.
IV Compatibility
There is limited information regarding IV Compatibility of Bosentan in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- Bosentan has been given as a single dose of up to 2400 mg in normal volunteers, or up to 2000 mg/day for 2 months in patients, without any major clinical consequences. The most common side effect was headache of mild to moderate intensity. In the cyclosporine A interaction study, in which doses of 500 and 1000 mg twice daily of bosentan were given concomitantly with cyclosporine A, trough plasma concentrations of bosentan increased 30-fold, resulting in severe headache, nausea, and vomiting, but no serious adverse events. Mild decreases in blood pressure and increases in heart rate were observed.
- In the postmarketing period, there was one reported overdose of 10,000 mg of Tracleer taken by an adolescent male patient. He had symptoms of nausea, vomiting, hypotension, dizziness, sweating, and blurred vision. He recovered within 24 hours with blood pressure support.
Management
- Bosentan is unlikely to be effectively removed by dialysis due to the high molecular weight and extensive plasma protein binding.
Chronic Overdose
There is limited information regarding Chronic Overdose of Bosentan in the drug label.
Pharmacology

| |
Bosentan
| |
| Systematic (IUPAC) name | |
| N-[6-(2-hydroxyethoxy)-5- (2-methoxyphenoxy) -2-pyrimidin-2-yl-pyrimidin-4-yl] -4-tert- butyl-benzenesulfonamide | |
| Identifiers | |
| CAS number | |
| ATC code | C02 |
| PubChem | |
| DrugBank | |
| Chemical data | |
| Formula | Template:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox |
| Mol. mass | 551.615 g/mol |
| SMILES | & |
| Pharmacokinetic data | |
| Bioavailability | 50% |
| Protein binding | >98% |
| Metabolism | Hepatic |
| Half life | 5 hours |
| Excretion | ? |
| Therapeutic considerations | |
| Pregnancy cat. |
X |
| Legal status |
Template:Unicode Prescription only |
| Routes | Oral |
Mechanism of Action
- Bosentan is a specific and competitive antagonist at endothelin receptor types ETA and ETB. Bosentan has a slightly higher affinity for ETA receptors than for ETB receptors. The clinical impact of dual endothelin blockage is unknown.
- Endothelin-1 (ET-1) is a neurohormone, the effects of which are mediated by binding to ETA and ETB receptors in the endothelium and vascular smooth muscle. ET-1 concentrations are elevated in plasma and lung tissue of patients with pulmonary arterial hypertension, suggesting a pathogenic role for ET-1 in this disease.
Structure
- Tracleer is the proprietary name for bosentan, an endothelin receptor antagonist that belongs to a class of highly substituted pyrimidine derivatives, with no chiral centers. It is designated chemically as 4-tert-butyl-N-[6-(2-hydroxy-ethoxy)-5-(2-methoxy-phenoxy)-[2,2´]-bipyrimidin-4-yl]- benzenesulfonamide monohydrate and has the following structural formula:
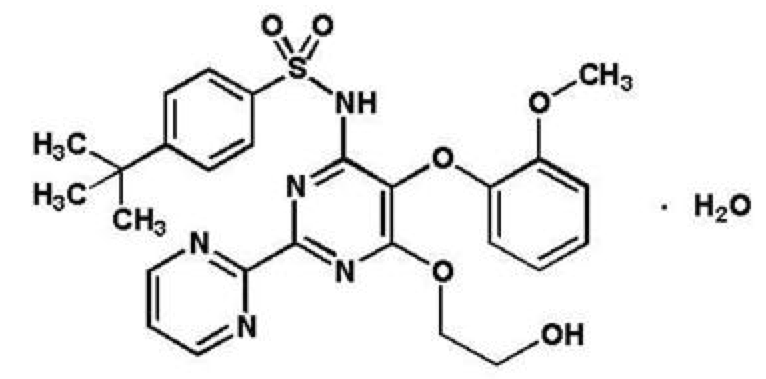
This image is provided by the National Library of Medicine.

- Bosentan has a molecular weight of 569.64 and a molecular formula of C27H29N5O6S•H2O. Bosentan is a white to yellowish powder. It is poorly soluble in water (1.0 mg/100 mL) and in aqueous solutions at low pH (0.1 mg/100 mL at pH 1.1 and 4.0; 0.2 mg/100 mL at pH 5.0). Solubility increases at higher pH values (43 mg/100 mL at pH 7.5). In the solid state, bosentan is very stable, is not hygroscopic and is not light sensitive.
- Tracleer is available as 62.5 mg and 125 mg film-coated tablets for oral administration, and contains the following excipients: corn starch, pregelatinized starch, sodium starch glycolate, povidone, glyceryl behenate, magnesium stearate, hydroxypropylmethylcellulose, triacetin, talc, titanium dioxide, iron oxide yellow, iron oxide red, and ethylcellulose. Each Tracleer 62.5 mg tablet contains 64.541 mg of bosentan, equivalent to 62.5 mg of anhydrous bosentan. Each Tracleer 125 mg tablet contains 129.082 mg of bosentan, equivalent to 125 mg of anhydrous bosentan.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Bosentan in the drug label.
Pharmacokinetics
General
- After oral administration, maximum plasma concentrations of bosentan are attained within 3–5 hours and the terminal elimination half-life (t1/2) is about 5 hours in healthy adult subjects. The exposure to bosentan after intravenous and oral administration is about 2-fold greater in adult patients with pulmonary arterial hypertension than in healthy adult subjects.
Absorption and Distribution
- The absolute bioavailability of bosentan in normal volunteers is about 50% and is unaffected by food. The volume of distribution is about 18 L. Bosentan is highly bound (> 98%) to plasma proteins, mainly albumin. Bosentan does not penetrate into erythrocytes.
Metabolism and Elimination
- Bosentan has three metabolites, one of which is pharmacologically active and may contribute 10%–20% of the effect of bosentan. Bosentan is an inducer of CYP2C9 and CYP3A and possibly also of CYP2C19. Total clearance after a single intravenous dose is about 4 L/hr in patients with pulmonary arterial hypertension. Upon multiple oral dosing, plasma concentrations in healthy adults decrease gradually to 50-65% of those seen after single dose administration, probably the effect of auto-induction of the metabolizing liver enzymes. Steady-state is reached within 3-5 days. Bosentan is eliminated by biliary excretion following metabolism in the liver. Less than 3% of an administered oral dose is recovered in urine.
Special Populations
- It is not known whether bosentan's pharmacokinetics is influenced by gender, race, or age.
Hepatic Impairment
- In vitro and in vivo evidence showing extensive hepatic metabolism of bosentan suggests that liver impairment could significantly increase exposure of bosentan. In a study comparing 8 patients with mild liver impairment (Child-Pugh Class A) to 8 controls, the single- and multiple-dose pharmacokinetics of bosentan was not altered in patients with mild hepatic impairment.
- In another small (N=8) pharmacokinetic study, the steady-state AUC of bosentan was on average 4.7 times higher and the active metabolite Ro 48-5033 was 12.4 times higher in 5 patients with moderately impaired liver function (Child-Pugh Class B) and pulmonary arterial hypertension associated with portal hypertension than in 3 patients with normal liver function and pulmonary arterial hypertension of other etiologies.
- The pharmacokinetics of Tracleer has not been evaluated in patients with severe liver impairment (Child-Pugh Class C).
Renal Impairment
- In patients with severe renal impairment (creatinine clearance 15–30 mL/min), plasma concentrations of bosentan were essentially unchanged and plasma concentrations of the three metabolites were increased about 2-fold compared to people with normal renal function. These differences do not appear to be clinically important.
Nonclinical Toxicology
Carcinogenesis and Mutagenesis
- Two years of dietary administration of bosentan to mice produced an increased incidence of hepatocellular adenomas and carcinomas in males at doses as low as 450 mg/kg/day (about 8 times the maximum recommended human dose [MRHD] of 125 mg twice daily, on a mg/m2 basis). In the same study, doses greater than 2000 mg/kg/day (about 32 times the MRHD) were associated with an increased incidence of colon adenomas in both males and females. In rats, dietary administration of bosentan for two years was associated with an increased incidence of brain astrocytomas in males at doses as low as 500 mg/kg/day (about 16 times the MRHD). In a comprehensive battery of in vitro tests (the microbial mutagenesis assay, the unscheduled DNA synthesis assay, the V-79 mammalian cell mutagenesis assay, and human lymphocyte assay) and an in vivo mouse micronucleus assay, there was no evidence for any mutagenic or clastogenic activity of bosentan.
Reproductive and Developmental Toxicology
- Bosentan was teratogenic in rats given oral doses ≥60 mg/kg/day. In an embryo-fetal toxicity study in rats, bosentan showed dose-dependent teratogenic effects, including malformations of the head, mouth, face and large blood vessels. Bosentan increased stillbirths and pup mortality at oral doses of 60 and 300 mg/kg/day. Although birth defects were not observed in rabbits given oral doses of up to 1500 mg/kg/day, plasma concentrations of bosentan in rabbits were lower than those reached in the rat. The similarity of malformations induced by bosentan and those observed in endothelin-1 knockout mice and in animals treated with other endothelin receptor antagonists indicates that teratogenicity is a class effect of these drugs.
Impairment of Fertility/Testicular Function
- The development of testicular tubular atrophy and impaired fertility has been linked with the chronic administration of certain endothelin receptor antagonists in rodents.
- Treatment with bosentan at oral doses of up to 1500 mg/kg/day (50 times the MRHD on a mg/m2 basis) or intravenous doses up to 40 mg/kg/day had no effects on sperm count, sperm motility, mating performance or fertility in male and female rats. An increased incidence of testicular tubular atrophy was observed in rats given bosentan orally at doses as low as 125 mg/kg/ day (about 4 times the MRHD and the lowest doses tested) for two years but not at doses as high as 1500 mg/kg/day (about 50 times the MRHD) for 6 months. Effects on sperm count and motility were evaluated only in the much shorter duration fertility studies in which males had been exposed to the drug for 4-6 weeks. An increased incidence of tubular atrophy was not observed in mice treated for 2 years at doses up to 4500 mg/kg/day (about 75 times the MRHD) or in dogs treated up to 12 months at doses up to 500 mg/kg/day (about 50 times the MRHD).
Clinical Studies
Pulmonary Arterial Hypertension
WHO Functional Class III-IV
- Two randomized, double-blind, multi-center, placebo-controlled trials were conducted in 32 and 213 patients. The larger study (BREATHE-1) compared 2 doses (125 mg twice daily and 250 mg twice daily) of Tracleer with placebo. The smaller study (Study 351) compared 125 mg twice daily with placebo. Patients had severe (WHO functional Class III–IV) pulmonary arterial hypertension: idiopathic or heritable pulmonary arterial hypertension (72%) or pulmonary arterial hypertension associated with scleroderma or other connective tissue diseases (21%), or to autoimmune diseases (7%). There were no patients with pulmonary arterial hypertension associated with other conditions such as HIV disease or recurrent pulmonary emboli.
- In both studies, Tracleer or placebo was added to patients' current therapy, which could have included a combination of digoxin, anticoagulants, diuretics, and vasodilators (e.g., calcium channel blockers, ACE inhibitors), but not epoprostenol. Tracleer was given at a dose of 62.5 mg twice daily for 4 weeks and then at 125 mg twice daily or 250 mg twice daily for either 12 (BREATHE-1) or 8 (Study 351) additional weeks. The primary study endpoint was 6-minute walk distance. In addition, symptoms and functional status were assessed. Hemodynamic measurements were made at 12 weeks in Study 351.
- The mean age was about 49 years. About 80% of patients were female, and about 80% were Caucasian. Patients had been diagnosed with pulmonary hypertension for a mean of 2.4 years.
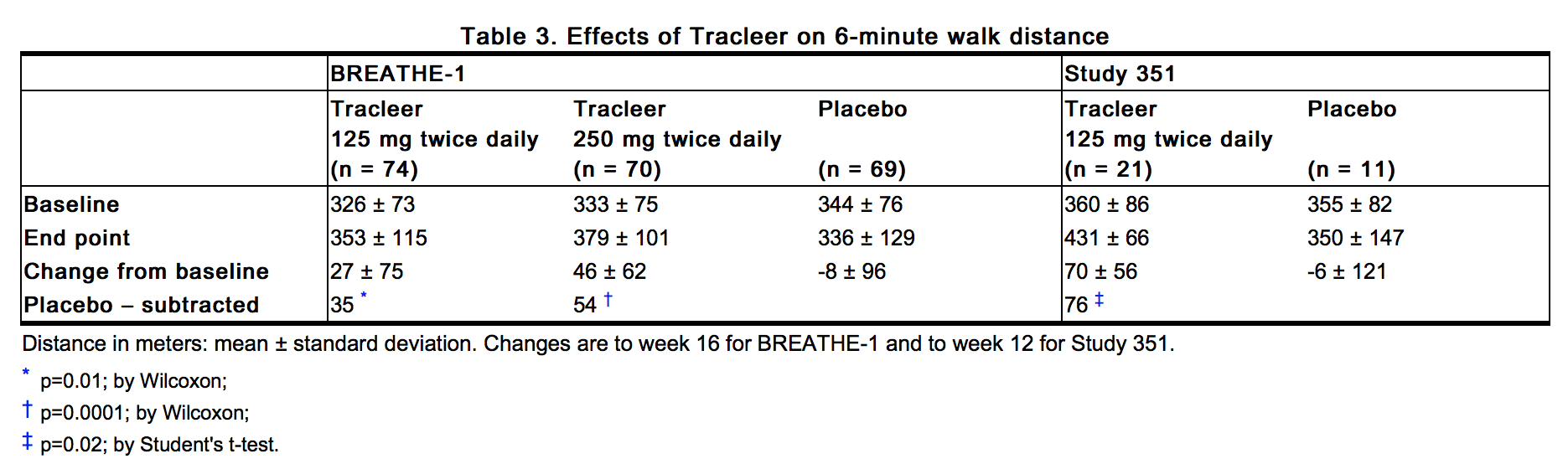
Submaximal Exercise Ability
- Results of the 6-minute walk distance at 3 months (Study 351) or 4 months (BREATHE-1) are shown in Table 3.
This image is provided by the National Library of Medicine.

- In both trials, treatment with Tracleer resulted in a significant increase in exercise ability. The improvement in walk distance was apparent after 1 month of treatment (with 62.5 mg twice daily) and fully developed by about 2 months of treatment (Figure 1). It was maintained for up to 7 months of double-blind treatment. Walking distance was somewhat greater with 250 mg twice daily, but the potential for increased hepatotoxicity causes this dose not to be recommended. There were no apparent differences in treatment effects on walk distance among subgroups analyzed by demographic factors, baseline disease severity, or disease etiology, but the studies had little power to detect such differences.

This image is provided by the National Library of Medicine.

- Change from baseline in 6-minute walking distance from start of therapy to week 16 in the placebo and combined Tracleer (125 mg twice daily and 250 mg twice daily) groups. Values are expressed as mean ± standard error of the mean.
Hemodynamic Changes
- Invasive hemodynamic parameters were assessed in Study 351. Treatment with Tracleer led to a significant increase in cardiac index (CI) associated with a significant reduction in pulmonary artery pressure (PAP), pulmonary vascular resistance (PVR), and mean right atrial pressure (RAP) (Table 4).
- The relationship between hemodynamic effects and improvements in 6-minute walk distance is unknown.

This image is provided by the National Library of Medicine.

Symptoms and Functional Status
- Symptoms of pulmonary arterial hypertension were assessed by Borg dyspnea score, WHO functional class, and rate of "clinical worsening." Clinical worsening was assessed as the sum of death, hospitalizations for PAH, discontinuation of therapy because of PAH, and need for epoprostenol. There was a significant reduction in dyspnea during walk tests (Borg dyspnea score), and significant improvement in WHO functional class in Tracleer-treated patients. There was a significant reduction in the rate of clinical worsening (Table 5 and Figure 2). Figure 2 shows the log-rank test reflecting clinical worsening over 28 weeks.

This image is provided by the National Library of Medicine. 
This image is provided by the National Library of Medicine.


WHO Functional Class II
- In a randomized, double-blind, multicenter, placebo-controlled trial, 185 mildly symptomatic PAH patients with WHO Functional Class II (mean baseline 6-minute walk distance of 443 meters) received Tracleer 62.5 mg twice daily for 4 weeks followed by 125 mg twice daily (n = 93), or placebo (n = 92) for 6 months. Enrolled patients were treatment-naïve (n = 156) or on a stable dose of sildenafil (n = 29). The coprimary endpoints were change from baseline to month 6 in PVR and 6-minute walk distance. Time to clinical worsening (assessed as the sum of death, hospitalization due to PAH complications, or symptomatic progression of PAH), Borg dyspnea index, change in WHO functional class and hemodynamics were assessed as secondary endpoints.
- Compared with placebo, Tracleer treatment was associated with a reduced incidence of worsening of at least one functional class (3% Tracleer vs. 13% placebo, p = 0.03), and improvement in hemodynamic variables (PVR, mPAP, TPR, cardiac index, and SVO2; p < 0.05). The + 19 m mean (+14 m median) increase in 6-minute walk distance with Tracleer vs. placebo was not significant (p = 0.08). There was a significant delay in time to clinical worsening (first seen primarily as symptomatic progression of PAH) with Tracleer compared with placebo (hazard ratio 0.2, p = 0.01). Findings were consistent in strata with or without treatment with sildenafil at baseline.
Long-term Treatment of PAH
- Long-term follow-up of patients with Class III and IV PAH who were treated with Tracleer in open-label extensions of trials (N=235) showed that 93% and 84% of patients were still alive at 1 and 2 years, respectively, after the start of treatment.
- These uncontrolled observations do not allow comparison with a group not given Tracleer and cannot be used to determine the long-term effect of Tracleer on mortality.
Pulmonary Arterial Hypertension related to Congenital Heart Disease with Left-to-Right Shunts
- A small study (N=54) and its open label extension (N=37) of up to 40 weeks with patients with Eisenmenger physiology demonstrated effects of Tracleer on exercise and safety that were similar to those seen in other trials in patients with PAH (WHO Group 1).
Lack of Benefit in Congestive Heart Failure
- Tracleer is not effective in the treatment of congestive heart failure with left ventricular dysfunction. In a pair of studies, 1613 subjects with NYHA Class III-IV heart failure, left ventricular ejection fraction <35%, on diuretics, ACE inhibitor, and other therapies, were randomized to placebo or Tracleer (62.5 mg twice daily titrated as tolerated to 125 mg twice daily) and followed for up to 70 weeks. Use of Tracleer was associated with no benefit on patient global assessment (the primary end point) or mortality. However, hospitalizations for heart failure were more common during the first 4 to 8 weeks after Tracleer was initiated. In a placebo-controlled trial of patients with severe chronic heart failure, there was an increased incidence of hospitalization for CHF associated with weight gain and increased leg edema during the first 4-8 weeks of treatment with Tracleer. Patients required intervention with a diuretic, fluid management, or hospitalization for decompensating heart failure.
How Supplied
- 62.5 mg film-coated, round, biconvex, orange-white tablets, embossed with identification marking "62,5", packaged in a white high-density polyethylene bottle and a white polypropylene child-resistant cap or in foil blister-strips for hospital unit-dosing.
- NDC 66215-101-06: Bottle containing 60 tablets.
- NDC 66215-101-03: Carton of 30 tablets in 10 blister strips of 3 tablets.
- 125 mg film-coated, oval, biconvex, orange-white tablets, embossed with identification marking "125", packaged in a white high-density polyethylene bottle and a white polypropylene child-resistant cap or in foil blister-strips for hospital unit-dosing.
- NDC 66215-102-06: Bottle containing 60 tablets.
- NDC 66215-102-03: Carton of 30 tablets in 10 blister strips of 3 tablets.
- Store at 20°C – 25°C (68°F – 77°F). Excursions are permitted between 15°C and 30°C (59°F and 86°F).
Storage
There is limited information regarding Bosentan Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Bosentan |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Bosentan |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information

Precautions with Alcohol
- Alcohol-Bosentan interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- Tracleer®[2]
Look-Alike Drug Names
- Tracleer® — Tricor®[3]
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Jaïs, Xavier (2008-12-16). "Bosentan for treatment of inoperable chronic thromboembolic pulmonary hypertension: BENEFiT (Bosentan Effects in iNopErable Forms of chronIc Thromboembolic pulmonary hypertension), a randomized, placebo-controlled trial". Journal of the American College of Cardiology. 52 (25): 2127–2134. doi:10.1016/j.jacc.2008.08.059. ISSN 1558-3597. PMID 19095129. Unknown parameter
|coauthors=ignored (help) - ↑ "TRACLEER (bosentan) tablet, film coated".
- ↑ "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Bosentan |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Bosentan |Label Name=Bosentan10.png
}}
{{#subobject:
|Label Page=Bosentan |Label Name=Bosentan11.png
}}
{{#subobject:
|Label Page=Bosentan |Label Name=Bosentan12.png
}}
 EncycloReader
is supported by the
EncycloReader
is supported by the