Fat necrosis
 From Wikidoc - Reading time: 4 min
From Wikidoc - Reading time: 4 min
| Fat necrosis | |
 | |
|---|---|
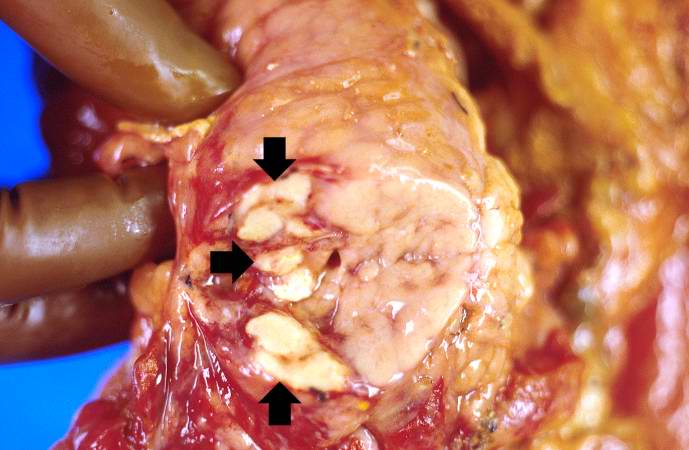
| This gross photograph shows the intestines and omentum at autopsy. Note the small (5-15 mm in diameter) white nodules on the surface of the omental and mesenteric fat tissue (arrows). Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology |
|
WikiDoc Resources for Fat necrosis |
|
Articles |
|---|
|
Most recent articles on Fat necrosis Most cited articles on Fat necrosis |
|
Media |
|
Powerpoint slides on Fat necrosis |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Fat necrosis at Clinical Trials.gov Clinical Trials on Fat necrosis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Fat necrosis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Fat necrosis Discussion groups on Fat necrosis Patient Handouts on Fat necrosis Directions to Hospitals Treating Fat necrosis Risk calculators and risk factors for Fat necrosis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Fat necrosis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
[edit | edit source]Fat necrosis is a focal area of destruction of fat tissue resulting from abnormal release of activated lipases.[1] [2]
Injury to the pancreas (infection, toxins, viruses, trauma, ischemia) causes release of activated pancreatic enzymes which liquefy fat cell membranes. The released lipases split the triglyceride esters contained within the fat cells and these released fatty acids combine with calcium to form the grossly visible chalky white nodules characteristic of fat necrosis.
Diagnostic Findings
[edit | edit source]Mammogram
[edit | edit source]- Mammographic spectrum of appearances of fat necrosis ranges from the characteristically benign to the potentially malignant.
- Calcifications seen at mammography may be clear-cut, benign rings, rims, or coarse macrocalcifications or may manifest as suspicious pleomorphic or even "branching type" microcalcifications.
Ultrasound
[edit | edit source]- Masses are most commonly solid, although they may be complex or cystic.
- Borders may be discrete or ill-defined.
- Posterior shadowing or enhancement may be present.
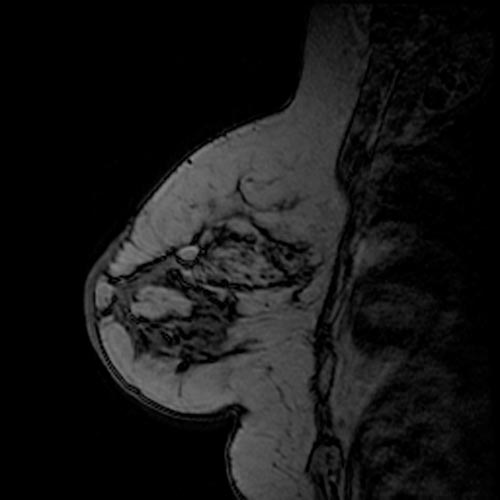
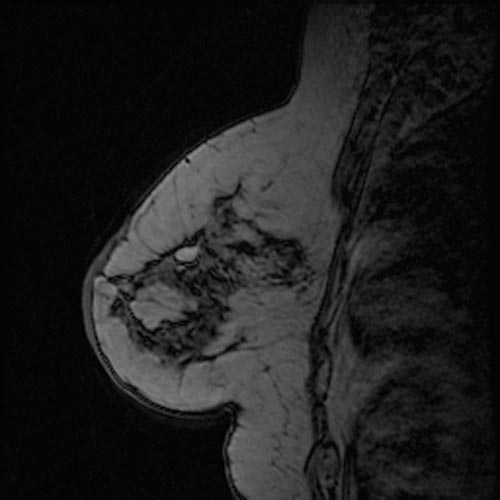
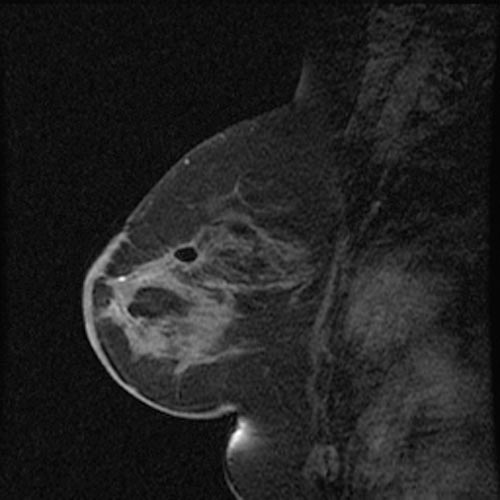
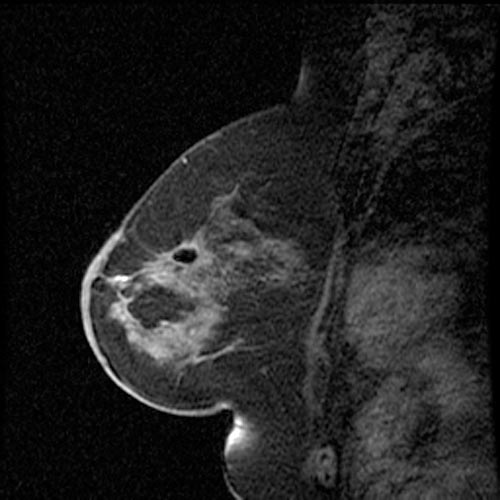
MRI
[edit | edit source]- Signal follows that of fat: Bright on T1 with loss of signal of fat saturated images.
-
 Fat necrosis
Fat necrosis -
 Fat necrosis
Fat necrosis -
 Fat necrosis
Fat necrosis -
 Fat necrosis
Fat necrosis




Pathological Findings: Case #1
[edit | edit source]Clinical Summary
[edit | edit source]A 37-year-old female with chronic renal failure that necessitated a renal transplant. Following transplantation, the patient developed a herpes simplex virus infection (HSV) in her nasal cavity, oral candidiasis, pneumonia, hematuria, pyuria, and gastrointestinal bleeding. Subsequently, the patient became septic and died.
Autopsy Findings
[edit | edit source]Major findings at autopsy included extensive hemorrhagic bronchopneumonia (Pseudomonas aeruginosa) and multiple ulcers affecting the stomach and esophagus. There was also evidence of disseminated intravascular coagulation (DIC) with multiple hemorrhages present. Firm, whitish foci of necrotic tissue were found in the fat around the pancreas.
-
 This gross photograph shows the intestines and omentum at autopsy. Note the small (5-15 mm in diameter) white nodules on the surface of the omental and mesenteric fat tissue (arrows).
This gross photograph shows the intestines and omentum at autopsy. Note the small (5-15 mm in diameter) white nodules on the surface of the omental and mesenteric fat tissue (arrows). -
 This gross photograph of the pancreas from this case shows white nodules (arrows) in the pancreas and the adjacent mesenteric fat tissue.
This gross photograph of the pancreas from this case shows white nodules (arrows) in the pancreas and the adjacent mesenteric fat tissue. -
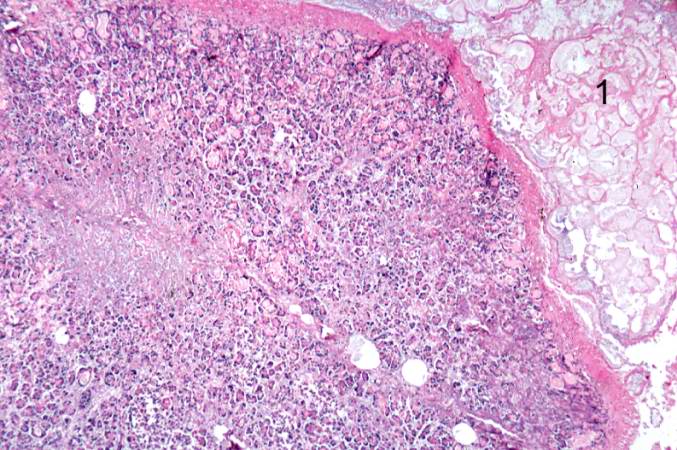
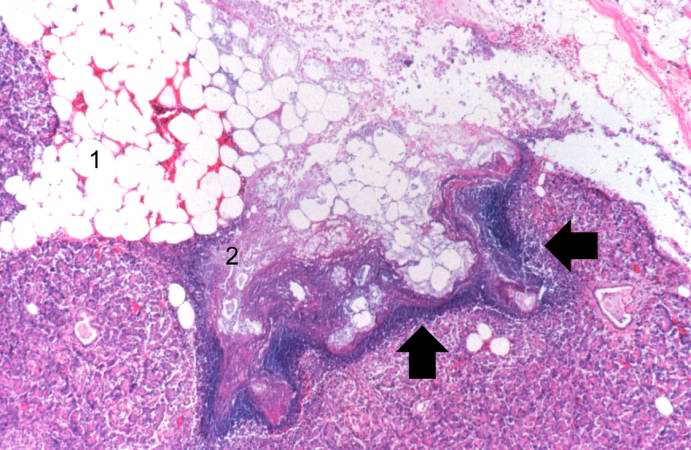 This low-power photomicrograph of the pancreas from this case shows the fat tissue (1) surrounding the pancreas. Note the rim of inflammatory cells (arrows) and the blue areas in the fat adjacent to the pancreas (2).
This low-power photomicrograph of the pancreas from this case shows the fat tissue (1) surrounding the pancreas. Note the rim of inflammatory cells (arrows) and the blue areas in the fat adjacent to the pancreas (2).


-
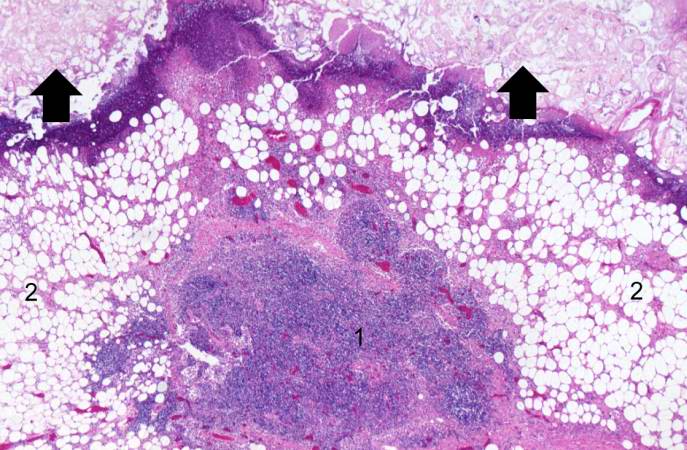 This high-power photomicrograph shows areas of inflammation (1) and fat necrosis (arrows) in the peripancreatic fat tissue (2) of the pancreas from this case.
This high-power photomicrograph shows areas of inflammation (1) and fat necrosis (arrows) in the peripancreatic fat tissue (2) of the pancreas from this case. -
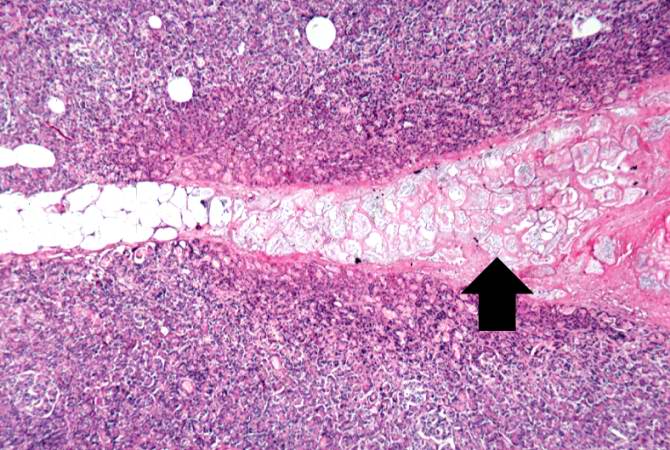
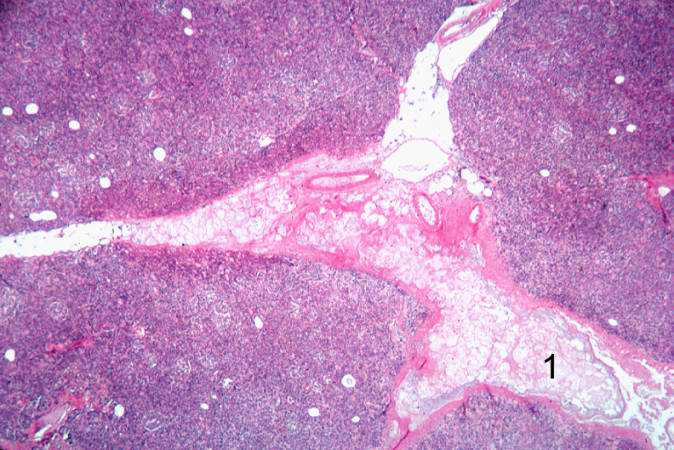 Another high-power photomicrograph shows blue discoloration in the fat tissue in the interlobular spaces (1) of the pancreas.
Another high-power photomicrograph shows blue discoloration in the fat tissue in the interlobular spaces (1) of the pancreas. -
 A higher-power photomicrograph of the previous slide contains a small area of fat necrosis (1) in the upper right portion of the image. The fat necrosis is within the fat tissue that is normally found adjacent to the pancreas. The appearance of the pancreatic tissue in this area is somewhat disrupted due to autolysis (the pancreas autolyzes very rapidly after death) but there is some premortem necrosis as well.
A higher-power photomicrograph of the previous slide contains a small area of fat necrosis (1) in the upper right portion of the image. The fat necrosis is within the fat tissue that is normally found adjacent to the pancreas. The appearance of the pancreatic tissue in this area is somewhat disrupted due to autolysis (the pancreas autolyzes very rapidly after death) but there is some premortem necrosis as well.



-
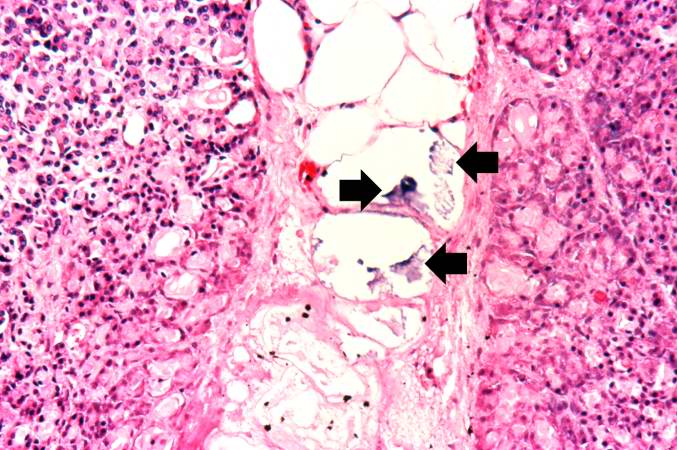
 This is a higher-power photomicrograph of the fat necrosis involving the fat cells in the interlobular spaces (arrow) of the pancreas. Note the blue to purple staining of the calcium deposits within the fat cells.
This is a higher-power photomicrograph of the fat necrosis involving the fat cells in the interlobular spaces (arrow) of the pancreas. Note the blue to purple staining of the calcium deposits within the fat cells. -
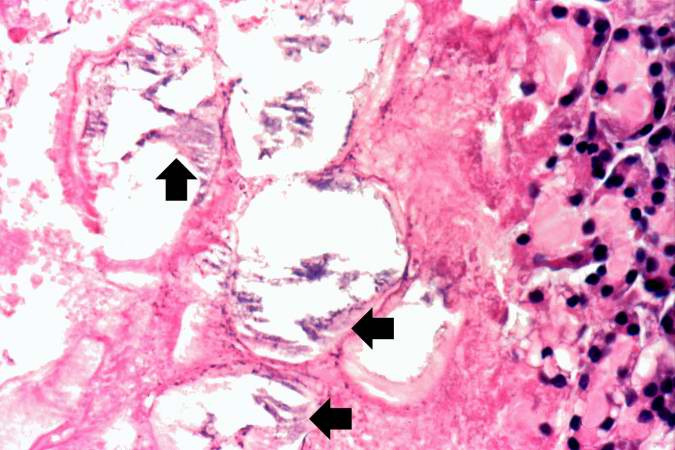
 This high-power photomicrograph demonstrates fat necrosis in the interlobular spaces of the pancreas. Note the granular blue-staining calcium deposits (arrows) within the fat cells. The clear areas represent artifact caused by the "washing-out" of fat from cells during tissue processing for histology.
This high-power photomicrograph demonstrates fat necrosis in the interlobular spaces of the pancreas. Note the granular blue-staining calcium deposits (arrows) within the fat cells. The clear areas represent artifact caused by the "washing-out" of fat from cells during tissue processing for histology. -
 This is another high-power photomicrograph demonstrating the calcification (arrows) seen in fat necrosis involving the interlobular spaces of the pancreas.
This is another high-power photomicrograph demonstrating the calcification (arrows) seen in fat necrosis involving the interlobular spaces of the pancreas.



References
[edit | edit source]- ↑ Dvora Cyrlak, and Philip M. Carpenter. Breast Imaging Case of the Day. RadioGraphics 1999 19: 80-83.
- ↑ JP Hogge, RE Robinson, CM Magnant, and RA Zuurbier. http://radiographics.rsnajnls.org/cgi/content/abstract/15/6/1347 The mammographic spectrum of fat necrosis of the breast.] RadioGraphics 1995 15: 1347-1356.
See Also
[edit | edit source]External Links
[edit | edit source] EncycloReader
is supported by the
EncycloReader
is supported by the