-
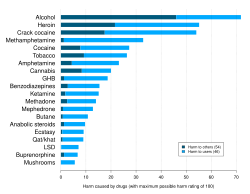 A 2010 study ranking various illegal and legal drugs based on statements by drug-harm experts in the UK. Crack cocaine and cocaine were found to be the third and fifth overall most dangerous drugs respectively.[85]
A 2010 study ranking various illegal and legal drugs based on statements by drug-harm experts in the UK. Crack cocaine and cocaine were found to be the third and fifth overall most dangerous drugs respectively.[85] -
 2007 delphic analysis regarding 20 popular recreational drugs based on expert opinion in the UK. Cocaine was ranked the 2nd in dependence and physical harm and 3rd in social harm.[86]
2007 delphic analysis regarding 20 popular recreational drugs based on expert opinion in the UK. Cocaine was ranked the 2nd in dependence and physical harm and 3rd in social harm.[86]
Table of Contents Categories
Cocaine
 From Wikipedia - Reading time: 110 min
From Wikipedia - Reading time: 110 min
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | kə(ʊ)ˈkeɪn |
| Trade names | Neurocaine,[1] Goprelto,[2] Numbrino,[3] others |
| AHFS/Drugs.com | Micromedex Detailed Consumer Information |
| License data | |
| Dependence liability | Physical: Low Psychological: High[4] |
| Addiction liability | High[5] |
| Routes of administration | Topical, by mouth, insufflation, intravenous, inhalation |
| Drug class | |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability |
|
| Metabolism | Liver, CYP3A4 |
| Metabolites | Norcocaine, benzoylecgonine, cocaethylene (when consumed with alcohol) |
| Onset of action | Seconds to minutes[13] |
| Duration of action | 20 to 90 minutes[13] |
| Excretion | Kidney |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| PDB ligand | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.000.030 |
| Chemical and physical data | |
| Formula | C17H21NO4 |
| Molar mass | 303.358 g·mol−1 |
| 3D model (JSmol) | |
| Melting point | 98 °C (208 °F) |
| Boiling point | 187 °C (369 °F) |
| Solubility in water | 1.8g/L (22 °C) |
| |
| |
| Data page | |
| Cocaine (data page) | |
| | |
Cocaine is a tropane alkaloid and central nervous system stimulant derived primarily from the leaves of two South American coca species: Erythroxylum coca and E. novogranatense, which are cultivated almost exclusively in the Andes.[14][15][16][17][18] Indigenous South Americans have used coca leaves for over a thousand years. Today, cocaine is rarely used medically, primarily as a topical medication, due to its high abuse potential, adverse effects, and high cost.[19][20] Recreational use is widespread, primarily due to its euphoric and aphrodisiac effects.[21][22]
Street cocaine is typically snorted, injected, or smoked as crack cocaine, with effects beginning within seconds to minutes and lasting up to 90 minutes depending on the route.[13][23] Pharmacologically, it is a serotonin–norepinephrine–dopamine reuptake inhibitor (SNDRI) that activates the mesolimbic pathway.[6][7][24][17] Intoxication may cause euphoria, psychosis, and physical symptoms like tachycardia and mydriasis.[13][25] An overdose can lead to stroke, heart attack, or sudden cardiac death.[17][26] Chronic cocaine use leads to cocaine dependence and can cause nose disorders, commonly referred to as "cocaine nose", including cocaine-induced midline destructive lesions (CIMDL) when insufflated.[27][28]
Large-scale chemical synthesis of cocaine is unexplored;[29] Instead, 99% of all global cocaine is made by first harvesting coca leaves by cocaleros from their coca plantations in the Andes. These leaves are then extracted into cocaine paste, which is subsequently processed into powdered hydrochloride salt.[18] Both the pharmaceutical supply chain and the illicit supply chain use all these steps, but they operate under very different controls and oversight. In Peru, for example, legal coca cultivation is monopolized by the state company National Coca Company (ENACO), yet approximately 90% of coca leaves produced in the country are diverted to illegal actors for cocaine manufacturing.[30] As a result, these illicit coca crops are a primary target of ongoing government-led coca eradication efforts.[31]
Cocaine is prohibited globally except for restricted medical and scientific uses under treaties like the Single Convention on Narcotic Drugs. Nevertheless, legal penalties vary by country. Some jurisdictions decriminalize possession of small amounts, leading to inconsistency in the legal status of cocaine worldwide.[32][33][34][35]
Uses
[edit]Coca leaves have been used by Andean civilizations since ancient times.[36] In ancient Wari culture,[37] Inca culture, and through modern successor indigenous cultures of the Andes mountains, coca leaves are chewed, taken orally in the form of a tea, or alternatively, prepared in a sachet wrapped around alkaline burnt ashes, and held in the mouth against the inner cheek; it has traditionally been used as an anorectic and to combat the effects of cold and altitude sickness,[38][39] although its actual effectiveness has never been systematically studied.[40]
Globally, in 2019, cocaine was used by an estimated 20 million people (0.4% of adults aged 15 to 64 years). The highest prevalence of cocaine use was in Australia and New Zealand (2.1%), followed by North America (2.1%), Western and Central Europe (1.4%), and South and Central America (1.0%).[41] Since 1961, the Single Convention on Narcotic Drugs has required countries to make recreational use of cocaine a crime.[42] In the United States, cocaine is regulated as a Schedule II drug under the Controlled Substances Act, meaning that it has a high potential for abuse but has an accepted medical use.[43] While rarely used medically today, its accepted uses include serving as a topical local anesthetic for the upper respiratory tract and as an antihemorrhagic agent to stop bleeding in the mouth, throat, and nasal cavities.[44]
Traditional
[edit]Coca leaves
[edit]
It is legal for people to use coca leaves in the Andean Community, such as Peru and Bolivia, where they are chewed, consumed in the form of tea, or are sometimes incorporated into food products.[45] Coca leaves are typically mixed with an alkaline substance (such as lime) and chewed into a wad that is retained in the buccal pouch (mouth between gum and cheek, much the same as chewing tobacco is chewed) and sucked of its juices. The juices are absorbed slowly by the mucous membrane of the inner cheek and by the gastrointestinal tract when swallowed.
Coca tea
[edit]
Coca herbal infusion (also referred to as coca tea) is used in coca-leaf producing countries much as any herbal medicinal infusion would elsewhere in the world. The free and legal commercialization of dried coca leaves under the form of filtration bags to be used as "coca tea" has been actively promoted by the governments of Peru and Bolivia for many years as a drink having medicinal powers. In Peru, the National Coca Company, a state-run corporation, sells cocaine-infused teas and other medicinal products and also exports leaves to the U.S. for medicinal use.[46] The effects of drinking coca tea are mild stimulation and mood lift.[47]
In 1986 an article in the Journal of the American Medical Association revealed that U.S. health food stores were selling dried coca leaves to be prepared as an infusion as "Health Inca Tea". While the packaging claimed it had been "decocainized", no such process had actually taken place. The article stated that drinking two cups of the tea per day gave a mild stimulation, increased heart rate, and mood elevation, and the tea was essentially harmless.[48]
Ypadu
[edit]
Ypadú or ypadu (also known as mambé) is an unrefined, unconcentrated powder made from toasted coca leaves and the ash of various other plants. It is traditionally prepared and consumed by indigenous tribes in the Northwest Amazon.[49] Like coca teas consumed in Peru to adapt to sickness induced by high elevation, it has a long ethnobotanical history and cultural associations.
Medical
[edit]Karl Koller’s groundbreaking discovery of cocaine as a local anesthetic is regarded as the second most significant advance in the history of anesthesia. Although cocaine was once widely preferred for topical anesthesia, the search for replacement agents intensified due to rising costs, strict regulations, and its habit-forming potential. Today, the US Drug Enforcement Administration (DEA) classifies cocaine as a Schedule II drug, recognizing its high potential for abuse but still permitting its limited use for medical purposes.
However, current pharmacoepidemiological trends suggest that cocaine may soon reach the point where, in practical terms, it is no longer used medically in health care as a Schedule II substance. This report may prompt some states (such as North Dakota) and institutions to reconsider whether further efforts to identify alternative agents are needed. As physician boards—but not pharmacy boards—continue to assess knowledge of licit cocaine, attention may shift toward drugs with more contemporary medical use.[20]
Cocaine is rarely prescribed in modern medicine due to its high potential for abuse and significant risk of adverse effects; its use is now almost exclusively limited to health facilities for specific diagnostic procedures or surgeries.
Topical
[edit]Cocaine is used in medical practice as a topical medication.[20] Because it is not absorbed into the bloodstream in significant amounts when used this way, topical application does not produce the psychoactive effects associated with recreational cocaine use.
Topical anesthetic
[edit]
Cocaine is sometimes used in otorhinolaryngology as a topical anesthetic and vasoconstrictor to help control pain and bleeding during surgery of the nose, mouth, throat, or lacrimal duct. It is also used for topical airway anaesthesia for procedures such as awake fibreoptic bronchoscopy or intubation. Although some absorption and systemic effects may occur, the use of cocaine as a topical anesthetic and vasoconstrictor is generally safe, rarely causing cardiovascular toxicity, glaucoma, and pupil dilation.[50][19] Occasionally, cocaine is mixed with adrenaline and sodium bicarbonate and used topically for surgery, a formulation called Moffett's solution.[51] It is occasionally used in surgeries involving the pharynx or nasopharynx to reduce pain, bleeding, and vocal cord spasm.[52]
Nasal solution cocaine hydrochloride (Goprelto), an ester used for intranasal application, was approved for medical use in the United States in December 2017, and is indicated for the introduction of topical anesthesia of the mucous membranes for diagnostic procedures and surgeries on or through the nasal cavities of adults.[53][2] Cocaine hydrochloride (Numbrino) was approved for medical use in the United States in January 2020.[54][3] Headache and epistaxis are the most frequently reported adverse reactions with Goprelto,[2] while hypertension and tachycardia-including sinus tachycardia-are most common with Numbrino.[3]
Ophthalmological use
[edit]Cocaine is an ophthalmological agent classified under ATC code S01HA Local anesthetics.
Cocaine eye drops are frequently used by neurologists when examining people suspected of having Horner syndrome. In Horner syndrome, sympathetic innervation to the eye is blocked. In a healthy eye, cocaine stimulates the sympathetic nervous system (SNS) by inhibiting norepinephrine reuptake, causing the pupil to dilate. In patients with Horner syndrome, sympathetic innervation to the eye is disrupted, so the affected pupil does not dilate in response to cocaine and remains constricted, or dilates to a lesser extent than the unaffected eye, which also receives the eye drop test. If both eyes dilate equally, the patient does not have Horner syndrome.[55]
Recreational
[edit]
Recreational cocaine is typically not taken by mouth due to its poor bioavailability, instead it is usually snorted, injected. Cocaine hydrochloride can also be chemically converted into its free base form, crack cocaine, which can be vaporized.
Cocaine is a central nervous system stimulant.[56] Its effects can last from 15 minutes to an hour. The duration of cocaine's effects depends on the amount taken and the route of administration.[57] Cocaine can be in the form of fine white powder and has a bitter taste. Crack cocaine is a smokeable form of cocaine made into small "rocks" by processing cocaine with sodium bicarbonate (baking soda) and water.[13][58]
Cocaine use leads to increases in alertness, feelings of well-being and euphoria, increased energy and motor activity, and increased feelings of competence and sexuality.[59]
Analysis of the correlation between the use of 18 various psychoactive substances shows that cocaine use correlates with other "party drugs" (such as ecstasy or amphetamines), as well as with heroin and benzodiazepines use, and can be considered as a bridge between the use of different groups of drugs.[60]
In 2023, David Liddell of the Scottish Drugs Forum reported a rise in cocaine use, particularly among people with long-term drug problems, and noted that stigma often delays users from seeking help until their issues become severe.[61]
Insufflation
[edit]
Nasal insufflation (known colloquially as "snorting", "sniffing", or "blowing") is a common method of ingestion of recreational powdered cocaine.[63] The drug coats and is absorbed through the mucous membranes lining the nasal passages. Cocaine's desired euphoric effects are delayed when snorted through the nose by about five minutes. This occurs because cocaine's absorption is slowed by its constricting effect on the blood vessels of the nose.[13] Insufflation of cocaine also leads to the longest duration of its effects (60–90 minutes).[13] When insufflating cocaine, absorption through the nasal membranes is approximately 30–60%[64]
In a study of cocaine users, the average time taken to reach peak subjective effects was 14.6 minutes.[65] Any damage to the inside of the nose is due to cocaine constricting blood vessels — and therefore restricting blood and oxygen/nutrient flow — to that area, which, after chronic use, may cause "cocaine nose."
Most banknotes have traces of cocaine on them; this has been confirmed by studies done in several countries.[66] In 1994, the U.S. 9th Circuit Court of Appeals cited findings that in Los Angeles, three out of four banknotes were tainted by cocaine or another illicit drug.[67][68]
Snuff spoons, hollowed-out pens, cut straws, pointed ends of keys,[69] long fingernails or artificial nails, and (clean) tampon applicators are also used to insufflate cocaine. The cocaine typically is poured onto a flat, hard surface (such as a mobile phone screen, plate, mirror, CD case or book) and divided into "bumps", "lines" or "rails", and then insufflated.[70] A 2001 study reported that the sharing of straws used to "snort" cocaine can spread blood diseases such as hepatitis C.[71]
Cocaine spoon
[edit].jpg)
Historically, snuff spoons were used for cocaine in the 20th century, hence the names "cocaine spoon" and "coke spoon". Some local statutes in the US treat spoons that are too small and thus "unsuited for the typical, lawful uses of a spoon" as drug paraphernalia.[72][73][74]
In the US, McDonald's provides straight swizzle sticks to stir the coffee, while in the rest of the world a small plastic stirring spoon is used. According to Anthony J. Graybosch, this is due to the 1960s rumor that the spoons can be used to snort cocaine.[75]
Injection
[edit]Subjective effects not commonly shared with other methods of administration include a ringing in the ears moments after injection (usually when over 120 milligrams) lasting 2 to 5 minutes including tinnitus and audio distortion. This is colloquially referred to as a "bell ringer". In a study of cocaine users, the average time taken to reach peak subjective effects was 3.1 minutes.[65] The euphoria passes quickly. Aside from the toxic effects of cocaine, there is also the danger of circulatory emboli from the insoluble substances that may be used to cut the drug. As with all injected illicit substances, there is a risk of the user contracting blood-borne infections if sterile injecting equipment is not available or used.
Inhalation
[edit]Crack cocaine
[edit]
Powder cocaine (cocaine hydrochloride) must be heated to a high temperature (about 197 °C), and considerable decomposition/burning occurs at these high temperatures. This effectively destroys some of the cocaine and yields a sharp, acrid, and foul-tasting smoke. Cocaine base/crack can be smoked because it vaporizes with little or no decomposition at 98 °C (208 °F),[76] which is below the boiling point of water.
Contraindications
[edit]Cocaine should not be used in individuals with a known allergy or hypersensitivity to the drug or any components of its topical formulation. It is also contraindicated in elderly patients and those with a history of hypertension or cardiovascular disease.[77]
Pregnancy
[edit]Under the former FDA pregnancy category system, cocaine was classified as a Category C drug. Its potential to cause harm to the fetus is not fully known, so it should only be administered to pregnant women if clearly necessary.[77]
Cocaine can act as a teratogen, having various effects on the developing fetus.[78] Some common teratogenic defects caused by cocaine include hydronephrosis, cleft palate, polydactyly, and down syndrome.[78] Cocaine as a drug has a low molecular weight and high water and lipid solubility which enables it to cross the placenta and fetal blood-brain barrier.[79] Because cocaine is able to pass through the placenta and enter the fetus, the fetus' circulation can be negatively affected. With restriction of fetal circulation, the development of organs in the fetus can be impacted, even resulting in intestines developing outside of the fetus' body.[78] Cocaine use during pregnancy can also result in obstetric labor complications such as premature labor,[80] placental abruption,[81] preterm birth or delivery, uterine rupture, miscarriage, and stillbirth.[78]
Breastfeeding
[edit]Mothers utilizing recreational drugs, such as cocaine, methamphetamines, PCP, and heroin, should not breastfeed.[82][83]: 13
The March of Dimes said "it is likely that cocaine will reach the baby through breast milk," and advises the following regarding cocaine use during pregnancy:
Cocaine use during pregnancy can affect a pregnant woman and her unborn baby in many ways. During the early months of pregnancy, it may increase the risk of miscarriage. Later in pregnancy, it can trigger preterm labor (labor that occurs before 37 weeks of pregnancy) or cause the baby to grow poorly. As a result, cocaine-exposed babies are more likely than unexposed babies to be born with low birth weight (less than 5.5 lb or 2.5 kg). Low-birthweight babies are 20 times more likely to die in their first month of life than normal-weight babies, and face an increased risk of lifelong disabilities such as mental retardation and cerebral palsy. Cocaine-exposed babies also tend to have smaller heads, which generally reflect smaller brains. Some studies suggest that cocaine-exposed babies are at increased risk of birth defects, including urinary tract defects and, possibly, heart defects. Cocaine also may cause an unborn baby to have a stroke, irreversible brain injury, or a myocardial infarction.[84]
Adverse effects
[edit]

Cardiac complications
[edit]Cocaine use can cause serious heart problems like sudden death, heart inflammation, arrhythmias, and heart attacks. It triggers coronary artery spasms, increases blood clot risk, and accelerates atherosclerosis, especially with long-term use. The severity of heart disease often relates to how long and how often cocaine is used.[87] It can also become a serious risk at high doses due to cocaine's blocking effect on cardiac sodium channels.[88]
Levamisole syndromes
[edit]Cocaine is frequently cut with levamisole.[89]
Levamisole induced necrosis syndrome
[edit]Levamisole induced necrosis syndrome (LINES) is a complication characterized by necrosis resulting from exposure to levamisole, a medication with immunomodulatory properties. While LINES can occur with levamisole use alone, most reported cases are associated with the use of cocaine adulterated with levamisole as a cutting agent. This syndrome is marked by skin necrosis, often affecting areas such as the ears, face, and extremities, and is thought to result from levamisole’s effects on blood vessels and the immune system.[90]
Cocaine/levamisole-associated syndromes
[edit]The skin necrosis associated with levamisole toxicity ranges from leukocytoclastic vasculitis to occlusive vasculopathy. Several cases of severe agranulocytosis associated with cocaine use have been reported since 2006. With the recently recognized dermal disease, the face and ears are commonly affected, especially the bilateral helices and cheeks. However, there have also been case reports of involvement of the abdomen, chest, lower buttocks and legs.[91][92]
During the mid-2010s, levamisole was found in most cocaine products available in both the United States and Europe.[93] Levamisole is known to cause an acute condition involving a severe and dangerous lowered white blood cell count, known as agranulocytosis, in cocaine users, and may also accentuate cocaine's effects.[94][95][96]
Cocaine- and levamisole-induced vasculitis
[edit]Cocaine- and levamisole-induced vasculitis (CLIV) is often used as an umbrella term for the vasculitic and necrotic complications seen with levamisole-adulterated cocaine, including both LINES and CLAAS.[97]
Cocaine and levamisole-adulterated cocaine (LAC) can cause cocaine-induced vasculitis (CIV) that mimics primary anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), presenting as cocaine-induced midline destructive lesions, LAC vasculopathy, or CIV. These conditions involve immune activation through NETosis and ANCA formation, leading to tissue damage. Diagnosis is challenging due to symptom overlap and undisclosed drug use, making clinical suspicion and drug history essential for proper management.[98]
Cocaine/levamisole-associated autoimmune syndrome
[edit]The broader cocaine/levamisole-associated autoimmune syndrome (CLAAS) includes LINES as a subset and is also common, but LINES is more specifically and frequently cited in the context of street cocaine adulteration.[99]
Levamisole has become a common additive to illicit cocaine. It is thought to intensify the "high" by releasing dopamine in the brain, acts as a bulking agent, and is a difficult adulterant to recognize. Potential risks of levamisole-laced cocaine include autoimmune disease, neutropenia, arthralgias, retiform purpura, skin necrosis, and fever.[100]
Mortality
[edit]Persons with regular or problematic use of cocaine have a significantly higher mortality rate, and are specifically at higher risk of traumatic deaths and deaths attributable to infectious disease.[101] In 2025, the Liberty House Clinic in the United Kingdom noted that chronic cocaine usage in fact had a higher risk of death than alcoholism.[102]
Neurotoxicity
[edit]Cocaine is considered neurotoxic due to its damaging effects on the brain and nervous system.[103][104][105] Research has shown that both acute and chronic cocaine use can lead to significant reductions in cerebral blood flow, disrupt neurovascular interactions, and impair brain function. These changes are associated with nerve injury, cognitive deficits, and an increased risk of cerebrovascular accidents such as strokes. Brain imaging studies consistently report that individuals who misuse cocaine exhibit structural and functional abnormalities compared to non-users, supporting the classification of cocaine as a neurotoxic substance.[103]
Psychosis
[edit]Cocaine has a similar potential to induce temporary psychosis[106] with more than half of cocaine abusers reporting at least some psychotic symptoms at some point.[107] Typical symptoms include paranoid delusions that they are being followed and that their drug use is being watched, accompanied by hallucinations that support the delusional beliefs.[107] Delusional parasitosis with formication ("cocaine bugs") is also a fairly common symptom.[108]
Cocaine-induced psychosis shows sensitization toward the psychotic effects of the drug. This means that psychosis becomes more severe with repeated intermittent use.[107][109]
Short-term effects
[edit]Insufflating (snorting) cocaine commonly causes increased mucus production due to irritation and inflammation of the nasal passages. This irritation leads to symptoms such as a runny nose, nasal congestion, and excessive or thickened mucus.
Acute exposure to cocaine has many effects on humans, including euphoria, increases in heart rate and blood pressure, and increases in cortisol secretion from the adrenal gland.[110] In humans with acute exposure followed by continuous exposure to cocaine at a constant blood concentration, the acute tolerance to the chronotropic cardiac effects of cocaine begins after about 10 minutes, while acute tolerance to the euphoric effects of cocaine begins after about one hour.[111][112][113][114] With excessive or prolonged use, the drug can cause itching, fast heart rate, and paranoid delusions or sensations of insects crawling on the skin.[115] Intranasal cocaine and crack use are both associated with pharmacological violence. Aggressive behavior may be displayed by both addicts and casual users. Cocaine can induce psychosis characterized by paranoia, impaired reality testing, hallucinations, irritability, and physical aggression. Cocaine intoxication can cause hyperawareness, hypervigilance, psychomotor agitation, and delirium. Consumption of large doses of cocaine can cause violent outbursts, especially by those with preexisting psychosis.[116] Acute exposure may induce arrhythmia, including atrial fibrillation, supraventricular tachycardia, ventricular tachycardia, and ventricular fibrillation. Acute exposure may also lead to angina, heart attack, and congestive heart failure.[117] Cocaine overdose may cause seizures, abnormally high body temperature and a marked elevation of blood pressure, which can be life-threatening,[115] abnormal heart rhythms,[88] and death.[88] Anxiety, paranoia, and restlessness can also occur, especially during the comedown. With excessive dosage, tremors, convulsions, and increased body temperature are observed.[56]
Long-term effects
[edit]
Cocaine is highly addictive and has poor bioavailability when taken orally. Individuals often engage in repeated use by either insufflating it intranasally or converting it to crack cocaine for vaporization. Cocaine's effects last longest when insufflated (60–90 minutes),[13] but the drug itself has a short biological half-life of about 0.7–1.5 hours.[118] Repeated use raises the risk of developing "cocaine nose," referring to severe nasal tissue damage from intranasal use, as well as "crack lung," a condition involving lung tissue damage caused by inhaling crack cocaine.
Cocaine use leads to an increased risk of hemorrhagic and ischemic strokes.[58] Cocaine use also increases the risk of having a heart attack.[119]
Cocaine use also promotes the formation of blood clots.[13] This increase in blood clot formation is attributed to cocaine-associated increases in the activity of plasminogen activator inhibitor, and an increase in the number, activation, and aggregation of platelets.[13]
Cocaine constricts blood vessels, dilates pupils, and increases body temperature, heart rate, and blood pressure. It can also cause headaches and gastrointestinal complications such as abdominal pain and nausea. Chronic users may lose their appetite and experience severe malnutrition, leading to being underweight.
Although it has been commonly asserted, the available evidence does not show that chronic use of cocaine is associated with broad cognitive impairment.[120] Research is inconclusive on age-related loss of striatal dopamine transporter (DAT) sites, suggesting cocaine has neuroprotective or neurodegenerative properties for dopamine neurons.[121][122][123] Exposure to cocaine may lead to the breakdown of the blood–brain barrier.[124][125]
The misuse of cocaine has a high correlation with suicide.[126][127] In those who use cocaine, the risk is greatest during the withdrawal phase.[128]
Chronic cocaine use, but not cocaine itself, can contribute to tooth wear and the development of tooth decay through indirect mechanisms.[clarification needed] Cocaine use is frequently associated with involuntary tooth grinding, known as bruxism, which can cause dental attrition and gingivitis.[129][130] Additionally, stimulants like cocaine, methamphetamine, and even caffeine cause dehydration and dry mouth. Since saliva is an important mechanism in maintaining one's oral pH level, people who use cocaine over a long period of time who do not hydrate sufficiently may experience demineralization of their teeth due to the pH of the tooth surface dropping too low (below 5.5). Poor oral hygiene, which is common among individuals with substance use disorders, may contribute significantly to tooth decay in cocaine users.[citation needed]
Addiction
[edit]Cocaine can induce tolerance after a single dose, and repeated use frequently leads to the development of addiction and prolonged craving.[111][131][132] Withdrawal symptoms include disrupted sleep, irritability, depression, and reduced ability to experience pleasure (anhedonia).[133][17] Chronic nasal use may cause destructive damage to the nasal septum, including cocaine-induced midline destructive lesions (CIMDL). Illicit cocaine is frequently adulterated with substances such as fentanyl, levamisole, or local anesthetics, increasing its toxicity.[36][134] Concurrent use with alcohol produces cocaethylene, a metabolite that significantly increases the risk of sudden death. According to the Global Burden of Disease Study, cocaine use is responsible for approximately 7,300 deaths annually.[135]
Cocaine abuse can trigger addiction-related structural neuroplasticity in the human brain, although the permanence of such changes remains uncertain.[136] Family history is a known risk factor, as relatives of cocaine users have an increased likelihood of developing cocaine addiction.[137] A key mechanism involves the overexpression of ΔFosB in the nucleus accumbens, altering transcriptional regulation and reinforcing drug-seeking behavior.[138] Each dose of cocaine raises ΔFosB levels without a known saturation point. This elevation leads to increased brain-derived neurotrophic factor (BDNF) levels, which in turn enhance dendritic branching and spine density in neurons of the nucleus accumbens and prefrontal cortex, potentially persisting for weeks after drug cessation.[citation needed]
In transgenic mice engineered to express ΔFosB in the nucleus accumbens and dorsal striatum, heightened behavioral sensitization to cocaine has been observed.[139] These mice self-administer cocaine at lower doses and display a greater propensity for relapse after withdrawal[140][141] ΔFosB also enhances sensitivity to reward by upregulating the AMPA receptor subunit GluR2[139] and downregulating the expression of dynorphin.[141]
Cocaine use has also been shown to increase DNA damage in the brains of rodents.[142][143] During subsequent DNA repair, enduring alterations in chromatin structure may arise, such as DNA methylation and methylation or acetylation of histones at the repair loci.[144] These modifications may result in lasting epigenetic "scars", which are believed to contribute to the persistent epigenetic changes observed in cocaine addiction.
Dependence and withdrawal
[edit]Cocaine dependence develops after even brief periods of regular cocaine use[145]
Cocaine withdrawal symptoms group into two types: depressive (e.g., depression, craving, insomnia) and somatic (e.g., increased appetite, fatigue). Depressive symptoms are linked to worse outcomes like longer depression, treatment, and risky behaviors.[146]
Treatment
[edit]Because there are no medications with an approved indication for cocaine use disorder, psychosocial treatments are the current standard. Effective approaches include group and individual counseling, cognitive behavioral therapy (CBT), and motivational interviewing (MI). Contingency management (CM)—which rewards patients with vouchers for meeting treatment goals—has proven especially effective, particularly for helping patients achieve initial abstinence from cocaine.[147]

Cocaine Anonymous (CA) is a twelve-step program formed in 18 November 1982 for people who seek recovery from drug addiction. It is patterned very closely after Alcoholics Anonymous (AA), although the two groups are unaffiliated. While many CA members have been addicted to cocaine, crack, speed or similar substances, CA accepts all who desire freedom from "cocaine and all other mind-altering substances" as members.[148]
Numerous medications have been investigated for use in cocaine dependence, but as of 2015[update], none of them were considered to be effective.[149] Drugs which help to re-stabilize the glutamate system such as N-acetylcysteine have been proposed for the treatment of addiction to cocaine, nicotine, and alcohol.[150] However, none have sufficient evidence or regulatory approval for routine clinical use, so psychosocial interventions remain the mainstay of treatment.[147]
Cocaine nose
[edit]
"Cocaine nose" or "coke nose" are informal terms that refer to nose disorders resulting from repeated or chronic cocaine use.[151][152][153][154]
About 30% of people who had snorted cocaine at least 25 times but less than daily, and 47% of daily users, reported experiencing nasal irritation, crusting or scabbing, and frequent nosebleeds. Cocaine use should be considered as a potential cause of persistent or unexplained rhinitis, including in adolescent patients.[155]
Because the nose is a prominent facial feature, such visible damage often leads to embarrassment, stigma, and negative reactions from others. As a result, individuals with cocaine-induced nasal damage frequently withdraw from social activities and relationships, leading to social isolation. In many cases, this isolation is not just likely but almost inevitable, as affected individuals may feel unable to face the outside world due to the noticeable and sometimes severe changes to their appearance.[156][157]
Nose disorders associated with cocaine nose include:
- Cocaine-induced midline destructive lesions (CIMDL)[27]
- Nasal septum perforation[28]
- Saddle nose[158]
Cocaine-induced midline destructive lesions
[edit]Cocaine-induced midline destructive lesions (CIMDL), colloquially known as "coke nose",[27] is the progressive destruction of nasal architecture with the erosion of the palate, nasal conchae, and ethmoid sinuses associated with prolonged insufflation, colloquially 'snorting', of cocaine.[28]
Chronic intranasal usage can degrade the cartilage separating the nostrils (the septum nasi), leading eventually to its complete disappearance.[159]
Causes
[edit]The cause of "cocaine nose" can be traced to the chemical process that occurs when cocaine hydrochloride is insufflated (snorted). As cocaine is absorbed through the nasal mucosa, the remaining hydrochloride component forms a dilute hydrochloric acid.[159] The short half-life of cocaine,[118] combined with binge use, may expose the nasal tissues to this acidic environment more frequently, increasing the risk of irritation and damage.
Treatment
[edit]For people with cocaine abuse, mild symptoms may resolve completely with total abstinence from cocaine, making early involvement of addiction services essential.[160]
Repair may involve rhinoplasty, which includes creating a new internal lining with nasolabial flaps and restoring support with costal cartilage grafts.[161]
In 2024, Belgian doctors report a rise in patients needing nose reconstruction due to cocaine use, which damages nasal tissue and cartilage; however, few undergo surgery because it requires at least six months of abstinence from cocaine for proper healing.[162]
Some individuals seek plastic surgery to repair or reconstruct nasal damage caused by cocaine use, although surgical outcomes can be complicated by ongoing tissue loss and poor healing. When nasal damage is too severe for reconstruction, a nose prosthesis may be used to restore appearance and quality of life.[156][157]
Overdose
[edit]

According to the European Union Drugs Agency, the estimated minimum lethal dose is 1.2 grams. However, sensitive individuals have died from as little as 30 milligrams applied to mucous membranes-an amount that is 40 times less than the minimum lethal dose. In contrast, addicts may tolerate doses as high as 5 grams per day.[14]
Cocaine can be snorted, swallowed, injected, or smoked. Most deaths due to cocaine are accidental but may also be the result of body packing or stuffing with rupture in the gastrointestinal tract. Alcohol impairment increases the likelihood of risk-taking behaviors and susceptibility to peer pressure, and also raises the risk of overdose due to the formation of cocaethylene (see the alcohol section).
Use of cocaine causes abnormally fast heart rhythms and a marked elevation of blood pressure (hypertension), which can be life-threatening. This can lead to death from acute myocardial infarction, acute respiratory failure (i.e., hypoxemia, with or without hypercapnia), stroke, cerebral hemorrhage, and sudden cardiac arrest.[164] Overdose can also cause acute hepatotoxicity—typically due to toxic metabolites—though most cases resolve quickly; however, fatal outcomes from multiple organ dysfunction syndrome are possible, and there is no specific antidote.[165] Cocaine overdose may result in hyperthermia as stimulation and increased muscular activity cause greater heat production. Heat loss is also inhibited by the cocaine-induced vasoconstriction.
In 2024, drug-related deaths in England and Wales reached their highest level in three decades, with a notable increase in fatalities involving cocaine and experts urging urgent government intervention to address the crisis. Martin Powell, from the charity Transform, which campaigns for the legal regulation of drugs, suggested that the recent rise in cocaine-related deaths in the UK may be due to the increased purity of cocaine, leading users to consume it more frequently and alongside other substances.[166]
Interactions
[edit]Alcohol
[edit]Alcohol interacts with cocaine in vivo to produce cocaethylene, another psychoactive substance which may be substantially more cardiotoxic than either cocaine or alcohol by themselves.[167][168]
MAOIs
[edit]Monoamine oxidase inhibitors (MAOIs) should not be combined with other psychoactive substances (antidepressants, painkillers, stimulants, including prescribed, OTC and illegally acquired drugs, etc.) except under expert care.[citation needed]
Opioids
[edit]The opioid epidemic now involves more overdose deaths with both opioids and cocaine, especially among non-Hispanic Blacks who are twice as likely to die from combined opioid-stimulant overdoses compared to non-Hispanic whites. Cocaine-related deaths in Blacks are similar to opioid deaths in whites. Risk factors include young age, education, urban living, mental disorders, and stress. It remains unclear if co-use is intentional. Recent studies expand focus beyond heroin to all opioids, reflecting changing overdose patterns.[169]
Pharmacology
[edit]Pharmacokinetics
[edit]The extent of absorption of cocaine into the circulatory system after nasal insufflation is similar to that after oral ingestion. The rate of absorption after nasal insufflation is limited by cocaine-induced vasoconstriction of capillaries in the nasal mucosa. Onset of absorption after oral ingestion is delayed because cocaine is a weak base with a pKa of 8.6, and is thus in an ionized form that is poorly absorbed from the gastric acid and easily absorbed from the alkaline duodenum.[12] The rate and extent of absorption from inhalation of cocaine is similar or greater than with intravenous injection, as inhalation provides access directly to the capillary bed. The delay in absorption after oral ingestion may account for the popular belief that cocaine bioavailability from the stomach is lower than after insufflation. Compared with ingestion, the faster absorption of insufflated cocaine results in quicker attainment of maximum drug effects. Snorting cocaine produces maximum physiological effects within 40 minutes and maximum psychotropic effects within 20 minutes. Physiological and psychotropic effects from nasally insufflated cocaine are sustained for approximately 40–60 minutes after the peak effects are attained.[170]
Cocaine crosses the blood–brain barrier via both a proton-coupled organic cation antiporter[171][172] and (to a lesser extent) via passive diffusion across cell membranes.[173] As of September 2022, the gene or genes encoding the human proton-organic cation antiporter had not been identified.[174]
Cocaine has a short elimination half life of 0.7–1.5 hours and is extensively metabolized by plasma esterases and also by liver cholinesterases, with only about 1% excreted unchanged in the urine.[13] The metabolism is dominated by hydrolytic ester cleavage, so the eliminated metabolites consist mostly of benzoylecgonine (BE), the major metabolite, and other metabolites in lesser amounts such as ecgonine methyl ester (EME) and ecgonine.[175][13] Further minor metabolites of cocaine include norcocaine, p-hydroxycocaine, m-hydroxycocaine, p-hydroxybenzoylecgonine (pOHBE), and m-hydroxybenzoylecgonine.[176]
Depending on liver and kidney functions, cocaine metabolites are detectable in urine between three and eight days. Generally speaking benzoylecgonine is eliminated from someone's urine between three and five days. In urine from heavy cocaine users, benzoylecgonine can be detected within four hours after intake and in concentrations greater than 150 ng/mL for up to eight days later.[177]
Detection in the body
[edit]Body fluids
[edit]Cocaine and its major metabolites may be quantified in blood, plasma, or urine to monitor for use, confirm a diagnosis of poisoning, or assist in the forensic investigation of a traffic or other criminal violation or sudden death. Most commercial cocaine immunoassay screening tests cross-react appreciably with the major cocaine metabolites, but chromatographic techniques can easily distinguish and separately measure each of these substances. When interpreting the results of a test, it is important to consider the cocaine usage history of the individual, since a chronic user can develop tolerance to doses that would incapacitate a cocaine-naive individual, and the chronic user often has high baseline values of the metabolites in his system. Cautious interpretation of testing results may allow a distinction between passive or active usage, and between smoking versus other routes of administration.[178]
Hair
[edit]Hair analysis can detect cocaine metabolites in regular users until after the sections of hair grown during the period of cocaine use are cut or fall out.[179]
Pharmacodynamics
[edit]Cocaine acts as a serotonin–norepinephrine–dopamine reuptake inhibitor (SNDRI).[7][24] Cocaine increases levels of serotonin, norepinephrine, and dopamine in the synaptic cleft, leading to heightened post-synaptic activation, with dopamine contributing to euphoria and arousal, and the other monoamines enhancing additional effects.[7][180][181][182]
The pharmacodynamics of cocaine involve the complex relationships of neurotransmitters (inhibiting monoamine uptake in rats with ratios of about: serotonin:dopamine = 2:3, serotonin:norepinephrine = 2:5).[183][17] The most extensively studied effect of cocaine on the central nervous system is the blockade of the dopamine transporter protein. Dopamine neurotransmitter released during neural signaling is normally recycled via the transporter; i.e., the transporter binds the transmitter and pumps it out of the synaptic cleft back into the presynaptic neuron, where it is taken up into storage vesicles. Cocaine binds tightly at the dopamine transporter forming a complex that blocks the transporter's function. The dopamine transporter can no longer perform its reuptake function, and thus dopamine accumulates in the synaptic cleft. The increased concentration of dopamine in the synapse activates post-synaptic dopamine receptors, which makes the drug rewarding and promotes the compulsive use of cocaine.[184]
Cocaine affects certain serotonin (5-HT) receptors; in particular, it has been shown to antagonize the 5-HT3 receptor, which is a ligand-gated ion channel. An overabundance of 5-HT3 receptors is reported in cocaine-conditioned rats, though 5-HT3's role is unclear.[185] The 5-HT2 receptor (particularly the subtypes 5-HT2A, 5-HT2B and 5-HT2C) are involved in the locomotor-activating effects of cocaine.[186]
Cocaine has been demonstrated to bind as to directly stabilize the DAT transporter on the open outward-facing conformation. Further, cocaine binds in such a way as to inhibit a hydrogen bond innate to DAT. Cocaine's binding properties are such that it attaches so this hydrogen bond will not form and is blocked from formation due to the tightly locked orientation of the cocaine molecule. Research studies have suggested that the affinity for the transporter is not what is involved in the habituation of the substance so much as the conformation and binding properties to where and how on the transporter the molecule binds.[187]
Conflicting findings have challenged the widely accepted view that cocaine functions solely as a reuptake inhibitor. To induce euphoria an intravenous dose of 0.3-0.6 mg/kg of cocaine is required, which blocks 66-70% of DAT in the brain.[188] Re-administering cocaine beyond this threshold does not significantly increase DAT occupancy but still results in an increase of euphoria which cannot be explained by reuptake inhibition alone. This discrepancy is not shared with other dopamine reuptake inhibitors like bupropion, sibutramine, mazindol or tesofensine, which have similar or higher potencies than cocaine as dopamine reuptake inhibitors. Furthermore, a similar response-occupancy discrepancy has been observed with methylphenidate, which also stabilizes the dopamine transporter in an open outward-facing conformation.[189][190][191] These findings have evoked a hypothesis that cocaine may also function as a so-called "DAT inverse agonist" or "negative allosteric modifier of DAT" resulting in dopamine transporter reversal, and subsequent dopamine release into the synaptic cleft from the axon terminal in a manner similar to but distinct from amphetamines.[189]
Sigma receptors are affected by cocaine, as cocaine functions as a sigma ligand agonist.[192] Further specific receptors it has been demonstrated to function on are NMDA and the D1 dopamine receptor.[193]
Cocaine also blocks sodium channels, thereby interfering with the propagation of action potentials;[194][88] thus, like lignocaine and novocaine, it acts as a local anesthetic. It also functions on the binding sites to the dopamine and serotonin sodium dependent transport area as targets as separate mechanisms from its reuptake of those transporters; unique to its local anesthetic value which makes it in a class of functionality different from both its own derived phenyltropanes analogues which have that removed. In addition to this, cocaine has some target binding to the site of the κ-opioid receptor.[195][unreliable medical source?] Cocaine also causes vasoconstriction, thus reducing bleeding during minor surgical procedures. Recent research points to an important role of circadian mechanisms[196] and clock genes[197] in behavioral actions of cocaine.
Cocaine is known to suppress hunger and appetite by increasing co-localization of sigma σ1R receptors and ghrelin GHS-R1a cell surface receptors, thereby increasing ghrelin-mediated signaling of satiety[198] and possibly via other effects on appetitive hormones.[199]
Cocaine effects, further, are shown to be potentiated for the user when used in conjunction with new surroundings and stimuli, and otherwise novel environs.[200]
Chemistry
[edit]Forms
[edit]

In its purest form, cocaine is a white, pearly powder. As a tropane alkaloid, cocaine is a weak base and readily forms salts when combined with acids. The most commonly encountered form is the hydrochloride (HCl) salt, although other salts such as the sulfate (SO42−) and nitrate (NO3−) are occasionally observed. The solubility of these salts varies depending on their polarity; the hydrochloride salt is polar and highly soluble in water.[201]
Synthesis
[edit]The first structure elucidation and total synthesis of the cocaine molecule was accomplished by Richard Willstätter in 1898.[202] Willstätter’s synthesis involved constructing the cocaine structure from simpler precursors, notably via the intermediate tropinone. Subsequent significant contributions to understanding the synthetic pathway and stereochemistry were made by Robert Robinson and Edward Leete.
Cocaine contains four chiral centers (1R, 2R, 3S, and 5S), two of which are configurationally dependent, resulting in eight possible stereoisomers. The formation of inactive stereoisomers, along with various synthetic by-products, limits both the yield and purity of the final product.[203][204]
Although the chemical synthesis of cocaine is technically feasible, it is generally considered impractical due to its high cost, low efficiency, and challenges in stereoselective synthesis compared to extraction from natural plant sources. While domestic clandestine laboratories could theoretically reduce reliance on offshore production and international smuggling—as seen with illicit methamphetamine manufacture and synthetic production of cocaine remains rare. Large-scale commercial synthesis has not been explored.[29]
Biosynthesis
[edit]
The carbon atoms required for the synthesis of cocaine are derived from acetyl-CoA, by addition of two acetyl-CoA units to the N-methyl-Δ1-pyrrolinium cation.[205] The first addition is a Mannich-like reaction with the enolate anion from acetyl-CoA acting as a nucleophile toward the pyrrolinium cation. The second addition occurs through a Claisen condensation. This produces a racemic mixture of the 2-substituted pyrrolidine, with the retention of the thioester from the Claisen condensation. In formation of tropinone from racemic ethyl [2,3-13C2]4(Nmethyl-2-pyrrolidinyl)-3-oxobutanoate there is no preference for either stereoisomer.[206]

In cocaine biosynthesis, only the (S)-enantiomer can cyclize to form the tropane ring system of cocaine. The stereoselectivity of this reaction was further investigated through study of prochiral methylene hydrogen discrimination.[207] This is due to the extra chiral center at C-2.[208] This process occurs through an oxidation, which regenerates the pyrrolinium cation and formation of an enolate anion, and an intramolecular Mannich reaction. The tropane ring system undergoes hydrolysis, SAM-dependent methylation, and reduction via NADPH for the formation of methylecgonine. The benzoyl moiety required for the formation of the cocaine diester is synthesized from phenylalanine via cinnamic acid.[209] Benzoyl-CoA then combines the two units to form cocaine.
N-methyl-pyrrolinium cation
[edit]The biosynthesis begins with L-Glutamine, which is derived to L-ornithine in plants. The major contribution of L-ornithine and L-arginine as a precursor to the tropane ring was confirmed by Edward Leete.[210] Ornithine then undergoes a pyridoxal phosphate (PLP)-dependent decarboxylation to form putrescine. In some animals, the urea cycle derives putrescine from ornithine. L-ornithine is converted to L-arginine,[211] which is then decarboxylated via PLP to form agmatine. Hydrolysis of the imine derives N-carbamoylputrescine followed with hydrolysis of the urea to form putrescine. The separate pathways of converting ornithine to putrescine in plants and animals have converged. A SAM-dependent N-methylation of putrescine gives the N-methylputrescine product, which then undergoes oxidative deamination by the action of diamine oxidase to yield the aminoaldehyde. Schiff base formation confirms the biosynthesis of the N-methyl-Δ1-pyrrolinium cation.

Robert Robinson's acetonedicarboxylate
[edit]The biosynthesis of the tropane alkaloid is still not understood. Hemscheidt proposes that Robinson's acetonedicarboxylate emerges as a potential intermediate for this reaction.[212] Condensation of N-methylpyrrolinium and acetonedicarboxylate would generate the oxobutyrate.[which?] Decarboxylation leads to tropane alkaloid formation.

Reduction of tropinone
[edit]The reduction of tropinone is mediated by NADPH-dependent reductase enzymes, which have been characterized in multiple plant species.[213] These plant species all contain two types of the reductase enzymes, tropinone reductase I and tropinone reductase II. TRI produces tropine and TRII produces pseudotropine. Due to differing kinetic and pH/activity characteristics of the enzymes and by the 25-fold higher activity of TRI over TRII, the majority of the tropinone reduction is from TRI to form tropine.[214]

GMO synthesis
[edit]In 2022, a GMO produced N. benthamiana were discovered that were able to produce 25% of the amount of cocaine found in a coca plant.[215]
However, since N. benthamiana also naturally contains nicotine, separating the cocaine from nicotine and related alkaloids would be challenging.
Field analysis
[edit]

Personal cards-including ID cards and driver's licenses-are frequently swabbed by inspectors to detect drug residue, as these items are commonly used to prepare lines of cocaine. Swabbing can reveal traces of cocaine or other illicit substances, providing evidence of recent drug handling or use. This practice may be employed during security checks at border crossings.
A Newsbeat investigation found that "cocaine torches" used by UK police to detect cocaine use are ineffective on typical street cocaine, as independent lab tests showed they fail to make the drug fluoresce. Experts and drug charities criticized the devices, warning they can give false positives and waste resources, while police forces defended their use as a deterrent. The manufacturer says the torches only work on much purer forms of cocaine than are found on the street.[216][217]
Cocaine may be detected by law enforcement using the Scott reagent. The test can easily generate false positives for common substances and must be confirmed with a laboratory test.[218][219]
Approximate cocaine purity can be determined using 1 mL 2% cupric sulfate pentahydrate in dilute HCl, 1 mL 2% potassium thiocyanate and 2 mL of chloroform. The shade of brown shown by the chloroform is proportional to the cocaine content. This test is not cross sensitive to heroin, methamphetamine, benzocaine, procaine and a number of other drugs but other chemicals could cause false positives.[220]
Society and culture
[edit]Street names
[edit]Cocaine is sometimes referred to on the street as blow, coca, coke, crank, flake, snow, or soda cot. Slang terms for free base cocaine include crack or rock.[22]
Prevalence
[edit]
World annual cocaine consumption, as of 2000, stood at around 600 tonnes, with the United States consuming around 300 t, 50% of the total, Europe about 150 t, 25% of the total, and the rest of the world the remaining 150 t or 25%.[221] It is estimated that 1.5 million people in the United States used cocaine in 2010, down from 2.4 million in 2006.[13] Conversely, cocaine use appears to be increasing[when?] in Europe with the highest prevalences in Spain, the United Kingdom, Italy, and Ireland.[13]
The 2010 UN World Drug Report concluded that "it appears that the North American cocaine market has declined in value from US$47 billion in 1998 to US$38 billion in 2008. Between 2006 and 2008, the value of the market remained basically stable".[222]
| Substance | Best estimate |
Low estimate |
High estimate |
|---|---|---|---|
| Amphetamine- type stimulants |
34.16 | 13.42 | 55.24 |
| Cannabis | 192.15 | 165.76 | 234.06 |
| Cocaine | 18.20 | 13.87 | 22.85 |
| Ecstasy | 20.57 | 8.99 | 32.34 |
| Opiates | 19.38 | 13.80 | 26.15 |
| Opioids | 34.26 | 27.01 | 44.54 |
According to a 2016 United Nations report, England and Wales are the countries with the highest rate of cocaine usage (2.4% of adults in the previous year).[224] Other countries where the usage rate meets or exceeds 1.5% are Spain and Scotland (2.2%), the United States (2.1%), Australia (2.1%), Uruguay (1.8%), Brazil (1.75%), Chile (1.73%), the Netherlands (1.5%) and Ireland (1.5%).[224]
Europe
[edit]Cocaine is the second most popular illegal recreational drug in Europe (behind cannabis). Since the mid-1990s, overall cocaine usage in Europe has been on the rise, but usage rates and attitudes tend to vary between countries.
Prevalence estimates for the general population: age ranges are 18-64 and 18-34 for Germany, Greece, France, Italy and Hungary; 16-64 and 16-34 for Denmark, Estonia and Norway; 18-65 for Malta; 17-34 for Sweden. Cocaine use in the general population is highest-ranging from 4.2% to 5.5%-in Denmark, Norway, Ireland, the Netherlands, in that order.[225]
South America
[edit]It is not widely recognized that South America is the world’s third largest market for cocaine use, with approximately 1,981,000 users as of 2004/5. The prevalence rate among people aged 15-64 stands at 0.7%, which is on par with Europe but significantly lower than North America’s 2.3%. In the main coca-producing countries, cocaine use rates are at or above the regional average, underscoring a strong connection between illicit crop cultivation, cocaine production, and local abuse. In Bolivia, where cocaine use is well above the Latin American average, annual prevalence rates have mirrored domestic production trends: after substantial increases in the early 1990s until 1996, rates declined, then began rising again from 2000 to 2005, reaching 1.6% for cocaine hydrochloride and 1.9% for cocaine base in 2005.[226]
United States
[edit]Cocaine is the second most popular illegal recreational drug in the United States (behind cannabis)[227] and the U.S. is the world's largest consumer of cocaine.[228] Its users span over different ages, races, and professions. In the 1970s and 1980s, the drug became particularly popular in the disco culture as cocaine usage was very common and popular in many discos such as Studio 54.
Legal status
[edit]
The production, distribution, and sale of cocaine products is restricted (and illegal in most contexts) in most countries as regulated by the Single Convention on Narcotic Drugs, and the United Nations Convention Against Illicit Traffic in Narcotic Drugs and Psychotropic Substances. In the United States the manufacture, importation, possession, and distribution of cocaine are additionally regulated by the 1970 Controlled Substances Act.
Some countries, such as Bolivia, Colombia, and Peru, permit the cultivation of coca leaf for traditional consumption by the local indigenous population, but nevertheless, prohibit the production, sale, and consumption of cocaine.[229] The provisions as to how much a coca farmer can yield annually is protected by laws such as the Bolivian Cato accord.[230] In addition, some parts of Europe, the United States, and Australia allow processed cocaine for medicinal uses only.
Australia
[edit]Cocaine is a Schedule 8 controlled drug in Australia under the Poisons Standard.[231] It is the second most popular illicit recreational drug in Australia behind cannabis.[232]
In Western Australia under the Misuse of Drugs Act 1981 4.0g of cocaine is the amount of prohibited drugs determining a court of trial, 2.0g is the amount of cocaine required for the presumption of intention to sell or supply and 28.0g is the amount of cocaine required for purposes of drug trafficking.[233]
United States
[edit]
The US federal government instituted a national drug labelling requirement for cocaine and cocaine-containing products through the Pure Food and Drug Act of 1906.[234]: 37 The next important federal regulation was the Harrison Narcotics Tax Act of 1914. While this act is often seen as the start of prohibition, the act itself was not actually a prohibition on cocaine, but instead set up a regulatory and licensing regime.[235] The Harrison Act did not recognize addiction as a treatable condition and therefore the therapeutic use of cocaine, heroin, or morphine to such individuals was outlawed – leading a 1915 editorial in the journal American Medicine to remark that the addict "is denied the medical care he urgently needs, open, above-board sources from which he formerly obtained his drug supply are closed to him, and he is driven to the underworld where he can get his drug, but of course, surreptitiously and in violation of the law."[236] The Harrison Act left manufacturers of cocaine untouched so long as they met certain purity and labeling standards.[234]: 40 Despite that cocaine was typically illegal to sell and legal outlets were rarer, the quantities of legal cocaine produced declined very little.[234]: 40 Legal cocaine quantities did not decrease until the Jones–Miller Act of 1922 put serious restrictions on cocaine manufactures.[234]: 40
Before the early 1900s, newspapers primarily portrayed addiction-not violence or crime-as the main problem caused by cocaine use, and depicted cocaine users as upper or middle class White people. In 1914, The New York Times published an article titled "Negro Cocaine 'Fiends' Are a New Southern Menace," portraying Black people who used cocaine as dangerous and able to withstand wounds that would normally be fatal.[237] The Anti-Drug Abuse Act of 1986 mandated the same prison sentences for distributing 500 grams of powdered cocaine and just 5 grams of crack cocaine.[238] In the National Survey on Drug Use and Health, white respondents reported a higher rate of powdered cocaine use, and Black respondents reported a higher rate of crack cocaine use.[239]
Harm reduction
[edit]
Experts recommend that anyone using stimulants such as cocaine or MDMA, as well as those around them, carry naloxone due to the growing risk of opioid contamination in the drug supply. Having naloxone available can help prevent fatal overdoses, even when opioids weren’t intentionally used.[240] Nasal spray formulations of naloxone are specifically recommended, as they are legal in many regions, easy to carry, and can be administered by anyone, not just medical professionals. The World Health Organization (WHO) includes naloxone on their "List of Essential Medicines", and recommends its availability and utilization for the reversal of opioid overdoses.[241][242] In the United States, some nasal naloxone are legally available without a prescription.[243][244]
Harm reduction efforts for cocaine use focus on reducing health risks associated with methods like cocaine injection and smoking crack cocaine. These include providing clean needles and crack cocaine paraphernalia, promoting safer consumption practices, and offering drug-checking services to detect dangerous contaminants such as fentanyl. Such strategies aim to minimize overdose risk and disease transmission while supporting users’ health and access to treatment, forming an essential part of modern drug policy.
Reagent testing
[edit]Reagent testing kits are widely used to identify the presence of cocaine and its common adulterants. The Scott reagent is specifically designed as a presumptive test for cocaine.[245] Morris reagent, which is derived from the Scott reagent, is also used as a presumptive test for cocaine. The Liebermann and Mandelin reagents are commonly used to test for both cocaine,[246][247] and levamisole, which is a frequent cutting agent found in street cocaine.[89]
Each reagent provides different color indications for various substances. Since adulteration of cocaine with levamisole is widespread, the color reactions produced by these reagents often reflect the presence of both substances. The resulting mixed color can complicate interpretation, making further analysis or additional testing necessary to clarify the sample’s composition.
DanceSafe recommends starting with Morris reagent to identify cocaine. A bright blue color means cocaine is present. Next, use Marquis reagent—no color change or light pink is normal, but orange may indicate amphetamines, so use a test strip if needed. Finally, test a fresh sample with Liebermann; yellow means pure cocaine, while rusty red suggests levamisole or lidocaine.[248]
Enforcement
[edit]Coca eradication
[edit].jpg)
Coca eradication is a strategy promoted by the United States government starting in 1961 as part of its "war on drugs" to eliminate the cultivation of coca, a plant whose leaves are not only traditionally used by indigenous cultures but also, in modern society, in the manufacture of cocaine. The strategy was adopted in place of running educational campaigns against drug usage.[249][unreliable source?] The prohibitionist strategy is being pursued in the coca-growing regions of Colombia (Plan Colombia), Peru, and formerly Bolivia, where it is highly controversial because of its environmental, health and socioeconomic impact. Furthermore, indigenous cultures living in the Altiplano, such as the Aymaras, use the coca leaf (which they dub the "millenary leaf") in many of their cultural traditions, notably for its medicinal qualities in alleviating the feeling of hunger, fatigue and headaches symptomatic of altitude sicknesses.[citation needed] The growers of coca are named Cocaleros and part of the coca production for traditional use is legal in Peru, Bolivia and Chile.[citation needed]
Interdiction
[edit]-
 U.S. Coast Guard Cutter Bertholf crewmembers offload approximately 14 tons of cocaine
U.S. Coast Guard Cutter Bertholf crewmembers offload approximately 14 tons of cocaine -
 United States CBP police inspect a seized shipment of cocaine.
United States CBP police inspect a seized shipment of cocaine. -
 1 kilo of cocaine seized from forwarded luggage at Innsbruck Airport
1 kilo of cocaine seized from forwarded luggage at Innsbruck Airport

.jpg)
.jpg)
The Consolidated Counterdrug Database (CCDB) is a U.S. government dataset created in the 1990s that compiles vetted data on cocaine trafficking and seizures in the Western Hemisphere "transit zone," involving 26 U.S. agencies and 20 foreign partners. It provides a highly reliable, conservative record of cocaine movements and interdiction efforts, revealing that despite large seizures, interdiction captures only a small fraction of trafficking events and has minimal impact on U.S. cocaine prices. The CCDB challenges optimistic views of drug interdiction effectiveness and underscores the need for new policy approaches, yet remains underutilized in research despite being unclassified.[250]
In 2004, according to the United Nations, 589 tonnes of cocaine were seized globally by law enforcement authorities. Colombia seized 188 t, the United States 166 t, Europe 79 t, Peru 14 t, Bolivia 9 t, and the rest of the world 133 t.[251]
Pharmaceutical supply chain
[edit]Production
[edit]Legal coca cultivation
[edit]In Bolivia, legal coca cultivation is regulated by the Coca and Integral Development agency, which operates under the Ministry of Rural Development.
In Colombia, the regulation of legal coca cultivation for traditional and scientific uses falls under the responsibility of government agencies, primarily the Ministry of Justice and Law (Ministerio de Justicia y del Derecho).
In Peru, The National Company of the Coca (Spanish: Empresa Nacional de la Coca, ENACO) is a state company dedicated to the commercialization of the coca leaf and derivatives. It is the only state company that has a monopoly on the commercialization and derivatives of the coca leaf. It was created in 1949.[252] In 1982, it became a state company under private law. Nonetheless, much of this cocaine enters the black market.[253] In 2023, one estimate was 90%.[254] The operation of the company is specified in Law 22095.
Stepan Company
[edit]The Stepan Company operates a unique facility in Maywood, New Jersey,[255] which is the only commercial plant in the United States authorized by the Drug Enforcement Administration to import and process coca leaves, primarily sourced from Peru via the National Coca Company. The Stepan Company extracts cocaine from the leaves, producing a cocaine-free coca extract that is supplied to The Coca-Cola Company for use as a flavoring ingredient in its beverages. The separated pharmaceutical-grade cocaine is sold to Mallinckrodt, a pharmaceutical company, for use in medical applications such as local anesthesia.[256]
Distribution
[edit]Mallinckrodt
[edit]As of 1988[update], Mallinckrodt is the only company in the U.S. that is allowed to receive cocaine, which is sold as a prescription drug for use in hospitals as a local anesthetic by eye and ear, nose and throat (ENT) doctors.[257]
Illicit supply chain
[edit]According to the United Nations Office on Drugs and Crime (UNODC), coca is cultivated almost exclusively in the Andean region, which spans the western edge of northern and central South America, with nearly all coca plantations located in Bolivia, Colombia, and Peru. The destruction of laboratories and production facilities demonstrates that most coca leaf processing into cocaine takes place near the cultivation areas in these countries. This includes both intermediate products, such as coca paste or base, and the final product, cocaine hydrochloride. UNODC further reports that over 99 percent of global cocaine production is concentrated in these three Andean countries.[18]
As a result, the global cocaine trade operates through a distinct illicit supply chain shaped by geography and economics. Production begins in South America, where coca plants are cultivated and processed through several chemical stages: first into a crude extract known as cocaine paste, then into coca base, and finally refined into cocaine hydrochloride. The drug is then trafficked-often across international borders-using a variety of smuggling routes and methods.
Although most cocaine paste and base are typically processed further within South America, there are cases where they are trafficked directly to other continents, such as Europe, for subsequent refinement into cocaine hydrochloride. In some instances, they are chemically embedded into materials like plastics to avoid detection.[226] Regardless of whether cocaine is incorporated into other chemicals—including cocaine hydrochloride—this method of concealment is referred to as "black cocaine".
After reaching consumer countries, cocaine enters distribution networks, where it is broken down into smaller quantities for local markets. Before reaching end users, the product is frequently adulterated, or “laced,” most commonly with the toxic stimulant levamisole to increase profits;[89] in some cases, counterfeit cocaine—substances sold as cocaine but containing little or no actual cocaine—is also distributed.[258] Finally, both genuine and adulterated cocaine products—those containing actual cocaine—as well as counterfeit cocaine (substances sold as cocaine but containing little or no actual cocaine) are sold at the retail level to consumers.
Production
[edit]
Colombia is as of 2019 the world's largest cocaine producer, with production more than tripling since 2013.[259][260] Three-quarters of the world's annual yield of cocaine has been produced in Colombia, both from cocaine base imported from Peru (primarily the Huallaga Valley) and Bolivia and from locally grown coca. There was a 28% increase in the amount of potentially harvestable coca plants which were grown in Colombia in 1998. This, combined with crop reductions in Bolivia and Peru, made Colombia the nation with the largest area of coca under cultivation after the mid-1990s. Coca grown for traditional purposes by indigenous communities, a use which is still present and is permitted by Colombian laws, only makes up a small fragment of total coca production, most of which is used for the illegal drug trade.[261]
| 2000 | 2001 | 2002 | 2003 | 2004 | |
|---|---|---|---|---|---|
| Net cultivation km2 (sq mi) | 1,875 (724) | 2,218 (856) | 2,007.5 (775.1) | 1,663 (642) | 1,662 (642) |
| Potential pure cocaine production (tonnes) | 770 | 925 | 830 | 680 | 645 |
The latest estimate provided by the U.S. authorities on the annual production of cocaine in Colombia refers to 290 metric tons. As of the end of 2011, the seizure operations of Colombian cocaine carried out in different countries have totaled 351.8 metric tons of cocaine, i.e. 121.3% of Colombia's annual production according to the U.S. Department of State's estimates.[263][264]
Overview
[edit]In 1991, the United States Department of Justice released a report detailing the typical process in which leaves from coca plants were ultimately converted into cocaine hydrochloride by Latin American drug cartels:[265]
- the exact species of coca to be planted was determined by the location of its cultivation, with Erythroxylum coca being grown in tropical high altitude climates of the eastern Andes in Peru and Bolivia, while Erythroxylum novogranatense was favoured in drier lowland areas of Colombia[265]
- the average cocaine alkaloid content of a sample of coca leaf varied between 0.1 and 0.8 percent, with coca from higher altitudes containing the largest percentages of cocaine alkaloids[265]
- the typical farmer will plant coca on a sloping hill so rainfall will not drown the plants as they reach full maturity over 12 to 24 months after being planted[265]
- the main harvest of coca leaves takes place after the traditional wet season in March, with additional harvesting also taking place in July and November[265]
- the leaves are then taken to a flat area and spread out on tarpaulins to dry in the hot sun for approximately 6 hours, and afterwards placed in 25 lb (11 kg) sacks to be transported to market or to a cocaine processing facility depending on location[265]
- in the early 1990s, Peru and Bolivia were the main locations for converting coca leaf to coca paste and cocaine base, while Colombia was the primary location for the final conversion for these products into cocaine hydrochloride[265]
- the conversion of coca leaf into coca paste was typically done very close to the coca fields to minimize the need to transport the coca leaves, with a plastic lined pit in the ground used as a "pozo"[265]
- the leaves are added to the pozo along with fresh water from a nearby river, along with kerosene and sodium carbonate, then a team of several people will repeatedly stomp on the mixture in their bare feet for several hours to help turn the leaves into paste[265]
- the cocaine alkaloids and kerosene eventually separate from the water and coca leaves, which are then drained off / scooped out of the mixture[265]
- the cocaine alkaloids are then extracted from the kerosene and added into a dilute acidic solution, to which more sodium carbonate is added to cause a precipitate to form[265]
- the acid and water are afterwards drained off and the precipitate is filtered and dried to produce an off-white putty-like substance, which is coca paste ready for transportation to cocaine base processing facility[265]
- at the processing facility, coca paste is dissolved in a mixture of sulfuric acid and water, to which potassium permanganate is then added and the solution is left to stand for 6 hours to allow the unwanted alkaloids to break down[265]
- the solution is then filtered and the precipitate is discarded, after which ammonia water is added and another precipitate is formed[265]
- when the solution has finished reacting the liquid is drained, then the remaining precipitate is dried under heating lamps, and resulting powder is cocaine base ready for transfer to a cocaine hydrochloride laboratory[265]
- at the laboratory, acetone is added to the cocaine base and after it has dissolved the solution is filtered to remove undesired material[265]
- hydrochloric acid diluted in ether is added to the solution, which causes the cocaine to precipitate out of the solution as cocaine hydrochloride crystals[265]
- the cocaine hydrochloride crystals are finally dried under lamps or in microwave ovens, then pressed into 1 kg (2.2 lb) blocks and wrapped in plastic ready for export[265]
Illegal coca cultivation
[edit]_Wellcome_V0043210.jpg)
Attempts to eradicate coca fields through the use of defoliants have devastated part of the farming economy in some coca-growing regions of Colombia, and strains appear to have been developed that are more resistant or immune to their use. Whether these strains are natural mutations or the product of human tampering is unclear. These strains have also shown to be more potent than those previously grown, increasing profits for the drug cartels responsible for the exporting of cocaine. Although production fell temporarily, coca crops rebounded in numerous smaller fields in Colombia, rather than the larger plantations.[266][267]
The cultivation of coca has become an attractive economic decision for many growers due to the combination of several factors, including the lack of other employment alternatives, the lower profitability of alternative crops in official crop substitution programs, the eradication-related damages to non-drug farms, the spread of new strains of the coca plant due to persistent worldwide demand.[268][269]
Clandestine chemistry
[edit]Cocaine paste
[edit]
In traditional cocaine production, solvents are key precursor chemicals used to extract and process cocaine from coca plant leaves. The process typically involves:
- Kerosene: Used to extract the cocaine alkaloid from the alkaline mixture of coca leaves and water.[14]
- Acetone, diethyl ether, ethyl acetate, chloroform: Used in later purification steps to dissolve or precipitate cocaine base or hydrochloride.[14]
Cocaine paste (paco, basuco, oxi, pasta) is a crude extract of the coca leaf which contains 40% to 91% cocaine freebase along with companion coca alkaloids and varying quantities of benzoic acid, methanol, and kerosene. In South America, coca paste—also known as cocaine base and often confused with cocaine sulfate in North America—is relatively inexpensive and widely used by working class consumers. The coca paste is smoked in tobacco or cannabis cigarettes and use has become widespread in several Latin American countries. Traditionally, coca paste has been relatively abundant in South American countries such as Colombia where it is processed into cocaine hydrochloride ("street cocaine") for distribution to the rest of the world.[270] The caustic reactions associated with the local application of coca paste prevents its use by oral, intranasal, mucosal, or injection routes. Coca paste can only be smoked when combined with a combustible material such as tobacco or cannabis.[271]
An interview with a coca farmer published in 2003 described a mode of production by acid-base extraction that has changed little since 1905. Roughly 625 pounds (283 kg) of leaves were harvested per hectare, six times per year. The leaves were dried for half a day, then chopped into small pieces with a string trimmer and sprinkled with a small amount of powdered cement (replacing sodium carbonate from former times). Several hundred pounds of this mixture were soaked in 50 US gallons (190 L) of gasoline for a day, then the gasoline was removed and the leaves were pressed for the remaining liquid, after which they could be discarded. Then battery acid (weak sulfuric acid) was used, one bucket per 55 lb (25 kg) of leaves, to create a phase separation in which the cocaine free base in the gasoline was acidified and extracted into a few buckets of "murky-looking smelly liquid". Once powdered caustic soda was added to this, the cocaine precipitated and could be removed by filtration through a cloth. The resulting material, when dried, was termed pasta and sold by the farmer. The 3,750 pounds (1,700 kg) yearly harvest of leaves from a hectare produced 6 lb (2.5 kg) of pasta, approximately 40–60% cocaine. Repeated recrystallization from solvents, producing pasta lavada and eventually crystalline cocaine were performed at specialized laboratories after the sale.[272]
Secondary extraction
[edit]Cocaine processing occurs in several EU Member States, with multiple laboratories dismantled annually. European cocaine processing often involves extracting cocaine that has been chemically concealed in materials like plastics, making detection in shipments challenging. Large quantities of cocaine base and paste are trafficked to Europe for conversion into cocaine hydrochloride. Each year, authorities detect some large-scale processing facilities; for example, six cocaine-processing labs were dismantled in Portugal between 2023 and 2024, resulting in the seizure of cocaine paste and cocaine hydrochloride.[226]
Trafficking
[edit]
Organized criminal gangs operating on a large scale dominate the cocaine trade. Most cocaine is grown and processed in South America, particularly in Colombia, Bolivia, Peru, and smuggled into the United States and Europe, the United States being the world's largest consumer of cocaine,[228] where it is sold at huge markups; usually in the US at $80–120 for 1 gram, and $250–300 for 3.5 grams (1/8 of an ounce, or an "eight ball").[273]
Smuggling methods
[edit]Concealment
[edit]-
 A 2,133-pound seizure of cocaine in a shipping container shipped from South America to Europe.
A 2,133-pound seizure of cocaine in a shipping container shipped from South America to Europe. -
 CBP seized 77 packages of cocaine and 34 packages of methamphetamine hidden in a hidden compartment in a cargo truck floor.
CBP seized 77 packages of cocaine and 34 packages of methamphetamine hidden in a hidden compartment in a cargo truck floor. -


.jpg)
.JPG)
Cocaine is frequently smuggled within shipping containers, mixed with legitimate cargo such as fruit, clothing, or canned goods. It is also commonly concealed in hidden compartments of vehicles and other objects, and criminal organizations have even created operational businesses to disguise drug shipments.
Additionally, cocaine is often concealed in a variety of everyday items and commercial goods to evade detection by authorities. Smugglers have hidden cocaine inside chocolate candies and other sweets, sometimes disguising the drug to look like ordinary candy bars or lollipops, which can be especially dangerous if accidentally consumed by children. Traffickers also use machinery and equipment-such as cotton-candy machines, construction equipment, and even heavy machinery parts-to hide cocaine, sometimes by impregnating the drug into materials like rubber or plastic components.
Black cocaine (Spanish: coca negra) is a form of cocaine in which the drug is mixed with various substances to disguise its appearance, interfere with color-based drug tests, and evade detection by drug-sniffing dogs; these additives may include pigments like charcoal, chemicals such as thiocyanates and iron or cobalt salts, and activated carbon to mask odors.
In 2024, Polish authorities seized 44 liters of liquid cocaine hidden in cartons of wine, valued at approximately 7.5 million zlotys ($1.85 million).[275]
Another commonality is creating an operational business to disguise the mass shipments.[276] Notorious drug lord Joaquin 'El Chapo' Guzman is one of many who have mixed legitimate business with their drug activities to conceal their illicit trading. El Chapo opened a cannery in Mexico and began producing canned jalapeños and peppers, and stuffed them with cocaine.[274]
At Miami International Airport in 1993, authorities discovered that some of the 312 boa constrictors in a shipment from Colombia had been surgically filled with condoms containing a total of 80 pounds (36 kg) of cocaine, resulting in the death of all the snakes.[277][278]
Mules
[edit]Mochileros (lit. 'backpackers') are drug couriers in the Latin American drug trade. They move drugs on foot from areas where it is produced, such as cocaine from the Valle de los Ríos Apurímac, Ene y Mantaro in Peru, to pick-up points from which it can be collected by the next link in the transport chain.[279] The work is highly dangerous.[279]
In Mexico, the people who engage in this type of activity are called "Burreros" (Spanish wordplay that refers to the person as a donkey, a pack animal), these people cross the border between Mexico and United States through the Sonoran Desert into Arizona. They usually trek through the desert in small groups, the journey taking more than a week to complete, each with a square-shaped package on their backs, containing around 55 pounds of illegal substances.[280]

.jpg)
Internationally, cocaine is also carried in small, concealed, kilogram quantities across the border by couriers known as "mules" (or "mulas"), who cross a border either legally, for example, through a port or airport, or illegally elsewhere. If the mule gets through without being caught, the gangs will receive most of the profits. If the mule is caught, gangs may sever all links and the mule will usually stand trial for trafficking alone.[281] In many cases, mules are often forced into the role, as result of coercion, violence, threats or extreme poverty.[281][282]
General smuggling techniques, which also have been used for cocaine, include:
- Concealment: Methods of smuggling include hiding the goods in a large vehicle in secret compartments,[283] luggage,[284] or clothes.[285]
- Body packing: The practice of transporting goods outside or inside of the body is called body packing.[286] This is done by a person usually called a mule or bait. The contraband is attached to the outside of the body using adhesive tape, glue, or straps, often in such places as between the cheeks of the buttocks or between rolls of fat.
- Swallowing: This is often done using a mule's gastrointestinal tract or other body cavities as containers.[287] In some cases, this has resulted in cardiac arrest.[288]
Maritime cocaine smuggling
[edit]Bulk cargo ships are also used to smuggle cocaine to staging sites in the Western Caribbean zone–Gulf of Mexico area. These vessels are typically 150–250-foot (50–80 m) coastal freighters that carry an average cocaine load of approximately 2.5 tonnes. Commercial fishing vessels are also used for smuggling operations. In areas with a high volume of recreational traffic, smugglers use the same types of vessels, such as go-fast boats, like those used by the local populations.[289][290]

Sophisticated drug subs are the latest tool drug runners are using to bring cocaine north from Colombia, it was reported on 20 March 2008. Although the vessels were once viewed as a quirky sideshow in the drug war, they are becoming faster, more seaworthy, and capable of carrying bigger loads of drugs than earlier models, according to those charged with catching them.[291]
In 2022, Spanish police seized three unmanned underwater vehicles used to smuggle drugs across the Strait of Gibraltar from Morocco, the first known interception of such devices. The drones, carrying up to 200 kg of narcotics each, were linked to French cartels. The operation led to eight arrests and exposed a gang using advanced drones and modified vehicles for trafficking across Europe (BBC, 2022).[292][293][294]
In 2025, international drug cartels began using sophisticated whale-shaped mini submarines to smuggle cocaine into Australia via Cyprus. These vessels are transported on cargo ships, dropped in international waters, then retrieved by smaller boats to deliver drugs ashore, posing a significant challenge to law enforcement detection efforts.[295]
Bribery
[edit]Bribery and corruption play a critical role in facilitating the illicit trafficking of cocaine. Drug trafficking organizations often rely on the bribery of government officials, law enforcement agents, customs officers, and border security personnel to evade detection and enable the smooth passage of cocaine shipments. These corrupt practices can involve payments, gifts, or other forms of illicit incentives aimed at securing cooperation or turning a blind eye to illegal activities.
Bribery helps traffickers circumvent checkpoints, avoid seizures, and reduce the risk of arrest or confiscation. It is particularly prevalent in regions with weak governance, limited law enforcement capacity, or endemic corruption, where officials may be more susceptible to financial inducements. This systemic corruption undermines efforts to combat drug trafficking and contributes to the persistence and expansion of cocaine supply chains.
Efforts to address bribery in the cocaine trade include international cooperation, anti-corruption initiatives, and strengthening institutional transparency and accountability. However, the clandestine nature of bribery makes it difficult to quantify its full impact on the illicit cocaine market.
Bribery has enabled cocaine trafficking in Hamburg’s port, with officials and insiders accepting illicit payments to facilitate smuggling. This corruption exposes systemic vulnerabilities despite Germany’s reputation for low corruption.[296][297][298]
Intercontinental distribution
[edit]Source regions
[edit]- Caribbean route

Cocaine traffickers from Colombia and Mexico have established a labyrinth of smuggling routes throughout the Caribbean, the Bahama Islands chain, and South Florida. They often hire traffickers from Mexico or the Dominican Republic to transport the drug using a variety of smuggling techniques to U.S. markets. These include airdrops of 500 to 700 kg (1,100 to 1,500 lb) in the Bahama Islands or off the coast of Puerto Rico, mid-ocean boat-to-boat transfers of 500 to 2,000 kg (1,100 to 4,400 lb), and the commercial shipment of tonnes of cocaine through the port of Miami.[299][300][301]
- Chilean route
Another route of cocaine traffic goes through Chile, which is primarily used for cocaine produced in Bolivia since the nearest seaports lie in northern Chile. The arid Bolivia–Chile border is easily crossed by 4×4 vehicles that then head to the seaports of Iquique and Antofagasta. While the price of cocaine is higher in Chile than in Peru and Bolivia, the final destination is usually Europe, especially Spain where drug dealing networks exist among South American immigrants.[302][303]
- Mexican route
The primary cocaine importation points in the United States have been in Arizona, Southern California, South Florida, and Texas. Typically, land vehicles are driven across the Mexico–United States border. As of 2006[update], sixty-five percent of cocaine enters the United States through Mexico, where the drug is first transported from South American countries.[304] As of 2015[update], the Sinaloa Cartel is the most active drug cartel involved in smuggling illicit drugs like cocaine into the United States and trafficking them throughout the United States.[305]
Destination hubs
[edit]- Hamburg
Hamburg, Germany’s largest port, has become a central hub for Europe’s cocaine trade, with record seizures—such as the 16-tonne bust in 2021—exposing deep institutional corruption as drug networks infiltrate police, justice, and port infrastructure; a lead prosecutor is currently on trial for allegedly leaking investigation details to traffickers in exchange for bribes, while insiders like dockworkers and security staff have enabled smuggling, highlighting how the staggering profits from cocaine are fueling violence, bribery, and systemic vulnerabilities in a country long considered among the least corrupt in the world.[296][297][298]
Wholesale distribution
[edit]After large-scale trafficking, cocaine is distributed within countries or regions by mid-level networks, primarily operating across major areas in both the United States and Europe.[226] These distributors break down bulk shipments into smaller quantities and supply local dealers or retail sellers. Distribution often involves organized groups that manage storage, transportation, and logistics to ensure the drug reaches various markets, preparing it for final sale to consumers.
Wholesale prices for cocaine increase dramatically as the drug moves from South America to consumer markets, with the cost in 2004 typically 15 times higher in the United States and 32 times higher in Europe than at the source in South America.[18]
Retail distribution
[edit]
Cocaine is readily available in all major countries' metropolitan areas. According to the Summer 1998 Pulse Check, published by the U.S. Office of National Drug Control Policy, cocaine use had stabilized across the country, with a few increases reported in San Diego, Bridgeport, Miami, and Boston. In the Western United States, cocaine usage was lower, which was thought to be due to a switch to methamphetamine among some users; methamphetamine is cheaper, three and a half times more powerful, and lasts 12–24 times longer with each dose.[306][307] Nevertheless, the number of cocaine users remain high, with a large concentration among urban youth.
In 2010, the purity- and inflation-adjusted retail price of cocaine was €191 per gram, based on data from 14 countries for which sufficient purity and price data were available, as reported by UNODC, ARQ, and EUROPOL.[308]
In addition to the amounts previously mentioned, cocaine can be sold in "bill sizes": As of 2007[update] for example, $10 might purchase a "dime bag", a very small amount (0.1–0.15 g) of cocaine. These amounts and prices are very popular among young people because they are inexpensive and easily concealed on one's body. Quality and price can vary dramatically depending on supply and demand, and on geographic region.[309]
In 2008, the European Monitoring Centre for Drugs and Drug Addiction reports that the typical retail price of cocaine varied between €50 and €75 per gram in most European countries, although Cyprus, Romania, Sweden, and Turkey reported much higher values.[310]
Lacing
[edit]
Street cocaine is often laced or "cut" with cheaper substances to increase bulk, including talc, lactose, sucrose, glucose, mannitol, inositol, caffeine, procaine, phencyclidine, phenytoin, lidocaine, strychnine, levamisole, fentanyl, and amphetamine.[312][313] Caffeine, often added to street cocaine, increases cocaine’s reinforcing and motivational effects, making the drug more compelling for users.[314]
Cocaine is rarely prescribed for medical use, so nearly all recreational cocaine is sourced illegally. As it moves through a long chain of traffickers—often a dozen or more—each looking to maximize profit, the drug is commonly mixed with various adulterants. This widespread adulteration significantly raises the risk of poisoning or overdose. For users, this means it is extremely difficult to know what substances have been added to the cocaine they purchase. Even when purity tests or reagent kits are used, these methods may not detect all possible contaminants or dangerous additives, making it nearly impossible to guarantee the drug's safety or purity.
The extent of cutting can vary significantly over time but for the last 15 years drugs such as cocaine ranged in Europe on average from 32% to 65% in purity.[315]
A problem with illegal cocaine use, especially in the higher volumes used to combat fatigue (rather than increase euphoria) by long-term users, is the risk of ill effects or damage caused by the compounds used in adulteration. Cutting or "stepping on" the drug is commonplace, using compounds which simulate ingestion effects, such as Novocain (procaine) producing temporary anesthesia, as many users believe a strong numbing effect is the result of strong and/or pure cocaine, ephedrine or similar stimulants that are to produce an increased heart rate. The normal adulterants for profit are inactive sugars, usually mannitol, creatine, or glucose, so introducing active adulterants gives the illusion of purity and to 'stretch' or make it so a dealer can sell more product than without the adulterants, however the purity of the cocaine is subsequently lowered.[316][317] The adulterant of sugars allows the dealer to sell the product for a higher price because of the illusion of purity and allows the sale of more of the product at that higher price, enabling dealers to significantly increase revenue with little additional cost for the adulterants. A 2007 study by the European Monitoring Centre for Drugs and Drug Addiction showed that the purity levels for street purchased cocaine was often under 5% and on average under 50% pure.[318]
Levamisole
[edit]Levamisole has increasingly been used as a cutting agent in cocaine sold around the globe with the highest incidence being in the United States. In 2008–2009, levamisole was found in 69% of cocaine samples seized by the Drug Enforcement Administration (DEA).[319] By April 2011, the DEA reported the adulterant was found in 82% of seizures.[320] By October 2017, this figure had risen further, with the DEA reporting that 87% of seized and analyzed cocaine bricks in the United States contained levamisole, making it the most common adulterant in cocaine at that time.[89]
In the body, levamisole is converted into aminorex, a toxic substance with amphetamine-like stimulant effects and a long duration of action.[321]
Cocaine acts as a serotonin–norepinephrine–dopamine reuptake inhibitor (SNDRI),[6][7] while aminorex is a serotonin–norepinephrine–dopamine releasing agent (SNDRA),[322][323][324] which is similar in that it increases the levels of these neurotransmitters but does so by promoting their release rather than inhibiting their reuptake.
Local anesthetics
[edit]Cocaine is sometimes cut with lidocaine,[325][326] and procaine.[327]
Opioids
[edit]Fentanyl has been increasingly found in cocaine samples.[312] In February 2022, 24 people in Argentina died after using cocaine laced with the fentanyl-analogue carfentanil.[328]
Nitazenes, a family of potent synthetic opioids, have also been detected.[329]
Counterfeit cocaine
[edit]The 2014 Amsterdam drug deaths underscore the dangers of misidentified drugs, as two tourists died after using heroin sold as cocaine.
In 2022, Canberra’s government-backed CanTEST drug checking clinic found that 40% of substances brought in as “cocaine” contained no cocaine at all. Instead, these samples were often made up of benign fillers such as dimethyl sulfone, highlighting significant adulteration in the local cocaine market. The actual cocaine samples tested also had low purity, with none exceeding 27%.[258][330]
Impact of illicit cocaine trade
[edit]Latin America
[edit]Drug war policies in Latin America and the Caribbean have led to more violence, higher incarceration rates, health crises, and deeper poverty, while undermining trust in institutions and worsening inequality. There is increasing support for shifting toward drug policies that focus on sustainable development and human rights instead of punitive measures.[331]
Research
[edit]Cocaine haptens are chemically modified derivatives of cocaine designed to retain the molecule’s immunogenic determinants while allowing for conjugation to carrier proteins. This enables the immune system to recognize and mount a response against cocaine.[332][333] By coupling cocaine haptens to carrier proteins (such as keyhole limpet hemocyanin or bovine serum albumin), researchers have developed vaccines that elicit the production of anti-cocaine antibodies. These antibodies can bind cocaine in the bloodstream, preventing it from reaching the brain and producing psychoactive effects.[334]
Coca tea has been promoted as an adjuvant for the treatment of cocaine dependence. One study on coca leaf infusion used with counseling in the treatment of 23 addicted coca-paste smokers in Lima, Peru found that the relapses rate fell from 4.35 times per month on average before coca tea treatment to one during treatment. The duration of abstinence increased from an average of 32 days before treatment to 217.2 days during treatment. This suggests that coca leaf infusion plus counseling may be effective at preventing relapse during cocaine addiction treatment.[335]
Recent research has also investigated the use of prescription psychostimulants as a treatment for cocaine dependence. This approach is consistent with the Self-Medication Hypothesis, which proposes that individuals may use cocaine to compensate for underlying neurochemical imbalances or psychological distress. Some studies suggest that psychostimulant therapy may help reduce cocaine use and cravings by addressing these underlying factors, though the evidence is mixed and further research is warranted.[336]
In mice, nicotine increased the probability of later consumption of cocaine, and the experiments permitted concrete conclusions on the underlying molecular biological alteration in the brain.[337] The biological changes in mice correspond to the epidemiological observations in humans that nicotine consumption is coupled to an increased probability of later use of cannabis and cocaine,[338] as well as other drugs.[339]
In rats, alcohol increased the probability of later addiction to cocaine and again relevant alterations in the reward system were identified.[340][341] These observations thus correspond to the epidemiological findings that the consumption of alcohol in humans is coupled to a later increased risk of a transition from cocaine use to cocaine addiction.[342][343]
Experimentally, cocaine injections can be delivered to animals such as fruit flies to study the mechanisms of cocaine addiction.[344]
TA-CD
[edit]TA-CD is a vaccine developed by the Xenova Group and designed to negate the effects of cocaine, making it suitable for use in treatment of addiction. It is created by combining norcocaine with inactivated cholera toxin.[345]
History
[edit]Discovery
[edit],_850-1500_C.E..jpg)
Indigenous peoples of South America have chewed the leaves of Erythroxylon coca—a plant that contains vital nutrients as well as numerous alkaloids, including cocaine—for over a thousand years.[346] The oldest evidence for the chewing of coca leaves dates back to c. 8000 B.C.E in Peru.[347] The coca leaf was, and still is, chewed almost universally by some indigenous communities. The remains of coca leaves have been found with ancient Peruvian mummies, and pottery from the time period depicts humans with bulged cheeks, indicating the presence of something on which they are chewing.[348] There is also evidence that these cultures used a mixture of coca leaves and saliva as an anesthetic for the performance of trepanation.[349]
When the Spanish arrived in South America, the conquistadors at first banned coca as an "evil agent of devil". But after discovering that without the coca the locals were barely able to work, the conquistadors legalized and taxed the leaf, taking 10% off the value of each crop.[350] In 1569, Spanish botanist Nicolás Monardes described the indigenous peoples' practice of chewing a mixture of tobacco and coca leaves to induce "great contentment":
When they wished to make themselves drunk and out of judgment they chewed a mixture of tobacco and coca leaves which make them go as they were out of their wittes.[351]
In 1609, Padre Blas Valera wrote:
Coca protects the body from many ailments, and our doctors use it in powdered form to reduce the swelling of wounds, to strengthen broken bones, to expel cold from the body or prevent it from entering, and to cure rotten wounds or sores that are full of maggots. And if it does so much for outward ailments, will not its singular virtue have even greater effect in the entrails of those who eat it?[352]
Isolation and naming
[edit]Although the stimulant and hunger-suppressant properties of coca leaves had been known for many centuries, the isolation of the cocaine alkaloid was not achieved until 1855. Various European scientists had attempted to isolate cocaine, but none had been successful for two reasons: the knowledge of chemistry required was insufficient, and conditions of sea-shipping from South America at the time would often degrade the quality of the cocaine in the plant samples available to European chemists by the time they arrived.[353] However, by 1855, the German chemist Friedrich Gaedcke successfully isolated the cocaine alkaloid for the first time.[354] Gaedcke named the alkaloid "erythroxyline", and published a description in the journal Archiv der Pharmazie.[355]
In 1856, Friedrich Wöhler asked Dr. Carl Scherzer, a scientist aboard the Novara (an Austrian frigate sent by Emperor Franz Joseph to circle the globe), to bring him a large amount of coca leaves from South America. In 1859, the ship finished its travels and Wöhler received a trunk full of coca. Wöhler passed on the leaves to Albert Niemann, a PhD student at the University of Göttingen in Germany, who then developed an improved purification process.[356]
Niemann described every step he took to isolate cocaine in his dissertation titled Über eine neue organische Base in den Cocablättern (On a New Organic Base in the Coca Leaves), which was published in 1860 and earned him his Ph.D. He wrote of the alkaloid's "colourless transparent prisms" and said that "Its solutions have an alkaline reaction, a bitter taste, promote the flow of saliva and leave a peculiar numbness, followed by a sense of cold when applied to the tongue." Niemann named the alkaloid "cocaine" from "coca" (from Quechua "kúka") + suffix "ine".[356][357]
The first synthesis and elucidation of the structure of the cocaine molecule was by Richard Willstätter in 1898.[202] It was the first biomimetic synthesis of an organic structure recorded in academic chemical literature.[358][359] The synthesis started from tropinone, a related natural product and took five steps.
Because of the former use of cocaine as a local anesthetic, a suffix "-caine" was later extracted and used to form names of synthetic local anesthetics.
Medicalization
[edit].jpg)


With the discovery of this new alkaloid, Western medicine was quick to exploit the possible uses of this plant.
In 1879, Vassili von Anrep, of the University of Würzburg, devised an experiment to demonstrate the analgesic properties of the newly discovered alkaloid. He prepared two separate jars, one containing a cocaine-salt solution, with the other containing merely saltwater. He then submerged a frog's legs into the two jars, one leg in the treatment and one in the control solution, and proceeded to stimulate the legs in several different ways. The leg that had been immersed in the cocaine solution reacted very differently from the leg that had been immersed in saltwater.[360]
Karl Koller (a close associate of Sigmund Freud, who would write about cocaine later) experimented with cocaine for ophthalmic usage. In an infamous experiment in 1884, he experimented upon himself by applying a cocaine solution to his own eye and then pricking it with pins. His findings were presented to the Heidelberg Ophthalmological Society. Also in 1884, Jellinek demonstrated the effects of cocaine as a respiratory system anesthetic. In 1885, William Halsted demonstrated nerve-block anesthesia,[361] and James Leonard Corning demonstrated peridural anesthesia.[362] 1898 saw Heinrich Quincke use cocaine for spinal anesthesia.
Although cocaine has traditionally been used for anesthesia in these procedures, substantial evidence shows it can cause severe and unpredictable toxic reactions, even with experienced practitioners. As a result, cocaine is no longer recommended for endonasal surgery. Safer and well-tolerated alternatives—such as lidocaine or tetracaine combined with agents like epinephrine, naphazoline, or oxymetazoline—are now preferred for topical and infiltration anesthesia.[19]
Popularization
[edit]In 1859, an Italian doctor, Paolo Mantegazza, returned from Peru, where he had witnessed first-hand the use of coca by the local indigenous peoples. He proceeded to experiment on himself and upon his return to Milan, he wrote a paper in which he described the effects. In this paper, he declared coca and cocaine (at the time they were assumed to be the same) as being useful medicinally, in the treatment of "a furred tongue in the morning, flatulence, and whitening of the teeth."
A chemist named Angelo Mariani who read Mantegazza's paper became immediately intrigued with coca and its economic potential. In 1863, Mariani started marketing a wine called Vin Mariani, which had been treated with coca leaves, to become coca wine. The ethanol in wine acted as a solvent and extracted the cocaine from the coca leaves, altering the drink's effect. It contained 6 mg cocaine per ounce of wine, but Vin Mariani which was to be exported contained 7.2 mg per ounce, to compete with the higher cocaine content of similar drinks in the United States.

In 1879 cocaine began to be used to treat morphine addiction. Cocaine was introduced into clinical use as a local anesthetic in Germany in 1884, about the same time as Sigmund Freud published his work Über Coca,[364] in which he wrote that cocaine causes:[365]
Exhilaration and lasting euphoria, which in no way differs from the normal euphoria of the healthy person. You perceive an increase of self-control and possess more vitality and capacity for work. In other words, you are simply normal, and it is soon hard to believe you are under the influence of any drug. Long intensive physical work is performed without any fatigue. This result is enjoyed without any of the unpleasant after-effects that follow exhilaration brought about by alcoholic beverages. No craving for the further use of cocaine appears after the first, or even after repeated taking of the drug.[366]
By 1885 the U.S. manufacturer Parke-Davis sold coca-leaf cigarettes and cheroots, a cocaine inhalant, a Coca Cordial, cocaine crystals, and cocaine solution for intravenous injection.[367] The company promised that its cocaine products would "supply the place of food, make the coward brave, the silent eloquent and render the sufferer insensitive to pain."

A "pinch of coca leaves" was included in John Styth Pemberton's original 1886 recipe for Coca-Cola, though the company began using decocainized leaves in 1906 when the Pure Food and Drug Act was passed. Today, Coca-Cola continues to use decocainized coca leaf extract for flavoring, which is processed by the Stepan Company in New Jersey; the leftover cocaine byproduct is sold for medical use.[368]
By the late Victorian era, cocaine use had appeared as a vice in literature. For example, it was injected by Arthur Conan Doyle's fictional Sherlock Holmes, generally to offset the boredom he felt when he was not working on a case.
In early 20th-century Memphis, Tennessee, cocaine was sold in neighborhood drugstores on Beale Street, costing five or ten cents for a small boxful. Dockworkers along the Mississippi River used the drug as a stimulant, and white employers encouraged its use by black laborers.[369]
In 1909, Ernest Shackleton took "Forced March" brand cocaine tablets to Antarctica, as did Captain Scott a year later on his ill-fated journey to the South Pole.[370]

In the 1931 song "Minnie the Moocher", Cab Calloway heavily references cocaine use. He uses the phrase "kicking the gong around", slang for cocaine use; describes titular character Minnie as "tall and skinny;" and describes Smokey Joe as "cokey".[371] In the 1932 comedy musical film The Big Broadcast, Cab Calloway performs the song with his orchestra and mimes snorting cocaine in between verses.[372]
During the mid-1940s, amidst World War II, cocaine was considered for inclusion as an ingredient of a future generation of 'pep pills' for the German military, code named D-IX.[373]
.jpg)
Cocaine Energy Supplement, also known as "Cocaine Energy Drink", is a highly caffeinated energy drink distributed by Hype Beverages.[374] Although the beverage contained no actual cocaine, the product launch attracted criticism from lawmakers and anti-drug organizations, who felt that Cocaine glamorized drug usage to children.[375][376]
Coca Colla is an energy drink produced in Bolivia with the use of coca extract as its base. It was launched on the Bolivian market in La Paz, Santa Cruz and Cochabamba in April 2010.[377][378]
In modern popular culture, references to cocaine are common. The drug has a glamorous image associated with the upper class, famous and powerful, and is said to make users "feel rich and beautiful".[379][380][381][382] In addition the pace of modern society − such as in finance − gives many the incentive to make use of the drug.[379]
Modern usage
[edit]
In many countries, cocaine is a popular recreational drug. Cocaine use is prevalent across all socioeconomic strata, including age, demographics, economic, social, political, religious, and livelihood.[383]
In the United States, the development of "crack" cocaine introduced the substance to a generally poorer inner-city market. The use of the powder form has stayed relatively constant, experiencing a new height of use across the 1980s and 1990s in the U.S.[384][385] However, from 2006 to 2010 cocaine use in the US declined by roughly half before again rising once again from 2017 onwards.[386] In the UK, cocaine use increased significantly between the 1990s and late 2000s, with a similar high consumption in some other European countries, including Spain.[387]
The estimated U.S. cocaine market exceeded US$70 billion in street value for the year 2005, exceeding revenues by corporations such as Starbucks.[388][389] Cocaine's status as a club drug shows its immense popularity among the "party crowd".[383]
In 1995 the World Health Organization (WHO) and the United Nations Interregional Crime and Justice Research Institute (UNICRI) announced in a press release the publication of the results of the largest global study on cocaine use ever undertaken. An American representative in the World Health Assembly banned the publication of the study, because it seemed to make a case for the positive uses of cocaine. An excerpt of the report strongly conflicted with accepted paradigms, for example, "that occasional cocaine use does not typically lead to severe or even minor physical or social problems." In the sixth meeting of the B committee, the US representative threatened that "If World Health Organization activities relating to drugs failed to reinforce proven drug control approaches, funds for the relevant programs should be curtailed". This led to the decision to discontinue publication. A part of the study was recuperated and published in 2010, including profiles of cocaine use in 20 countries, but are unavailable as of 2015[update].[390]
In October 2010 it was reported that the use of cocaine in Australia has doubled since monitoring began in 2003.[391]
Etymology
[edit]The word cocaine derives from French Cocaïne, from Spanish coca, ultimately from Quechua kúka.[392]
See also
[edit]- Cocaine reverse ester
- Cocaine and amphetamine regulated transcript
- MDMA – also acts, to a lesser extent, as an SNDRI like cocaine
References
[edit]- ^ Nordegren T (2002). The A-Z Encyclopedia of Alcohol and Drug Abuse. Universal-Publishers. p. 461. ISBN 978-1-58112-404-0. Archived from the original on 8 July 2024. Retrieved 3 September 2020.
- ^ a b c "Goprelto – cocaine hydrochloride solution". DailyMed. 3 January 2020. Archived from the original on 30 July 2020. Retrieved 30 April 2020.
- ^ a b c "Numbrino – cocaine hydrochloride nasal solution". DailyMed. 28 February 2020. Archived from the original on 30 July 2020. Retrieved 30 April 2020.
- ^ Ghodse H (2010). Ghodse's Drugs and Addictive Behaviour: A Guide to Treatment (4 ed.). Cambridge University Press. p. 91. ISBN 978-1-139-48567-8. Archived from the original on 10 September 2017.
- ^ Introduction to Pharmacology (3 ed.). Abingdon: CRC Press. 2007. pp. 222–223. ISBN 978-1-4200-4742-4. Archived from the original on 10 September 2017.
- ^ a b c Sora I, Hall FS, Andrews AM, Itokawa M, Li XF, Wei HB, et al. (April 2001). "Molecular mechanisms of cocaine reward: combined dopamine and serotonin transporter knockouts eliminate cocaine place preference". Proceedings of the National Academy of Sciences of the United States of America. 98 (9): 5300–5305. Bibcode:2001PNAS...98.5300S. doi:10.1073/pnas.091039298. PMC 33204. PMID 11320258.
- ^ a b c d e Azizi SA (April 2022). "Monoamines: Dopamine, Norepinephrine, and Serotonin, Beyond Modulation, "Switches" That Alter the State of Target Networks". The Neuroscientist. 28 (2): 121–143. doi:10.1177/1073858420974336. PMID 33292070. S2CID 228080727.
- ^ "DEA / Drug Scheduling". www.dea.gov. Archived from the original on 9 August 2017. Retrieved 7 August 2017.
- ^ a b Fattinger K, Benowitz NL, Jones RT, Verotta D (July 2000). "Nasal mucosal versus gastrointestinal absorption of nasally administered cocaine". European Journal of Clinical Pharmacology. 56 (4): 305–10. doi:10.1007/s002280000147. PMID 10954344. S2CID 20708443.
- ^ Barnett G, Hawks R, Resnick R (1981). "Cocaine pharmacokinetics in humans". Journal of Ethnopharmacology. 3 (2–3): 353–66. doi:10.1016/0378-8741(81)90063-5. PMID 7242115.
- ^ Jeffcoat AR, Perez-Reyes M, Hill JM, Sadler BM, Cook CE (1989). "Cocaine disposition in humans after intravenous injection, nasal insufflation (snorting), or smoking". Drug Metabolism and Disposition. 17 (2): 153–9. doi:10.1016/S0090-9556(25)08737-9. PMID 2565204.
- ^ a b Wilkinson P, Van Dyke C, Jatlow P, Barash P, Byck R (March 1980). "Intranasal and oral cocaine kinetics". Clinical Pharmacology and Therapeutics. 27 (3): 386–94. doi:10.1038/clpt.1980.52. PMID 7357795. S2CID 29851205.
- ^ a b c d e f g h i j k l m n Zimmerman JL (October 2012). "Cocaine intoxication". Critical Care Clinics. 28 (4): 517–26. doi:10.1016/j.ccc.2012.07.003. PMID 22998988.
- ^ a b c d "Cocaine and crack drug profile | www.euda.europa.eu". www.euda.europa.eu.
- ^ "Cocaine - Alcohol and Drug Foundation". adf.org.au.
- ^ "The identification of coca (Erythroxylum species)". Botanical Journal of the Linnean Society. doi:10.1111/j.1095-8339.1982.tb00368.x.
- ^ a b c d e Pomara C, Cassano T, D'Errico S, Bello S, Romano AD, Riezzo I, et al. (2012). "Data available on the extent of cocaine use and dependence: biochemistry, pharmacologic effects and global burden of disease of cocaine abusers". Current Medicinal Chemistry. 19 (33): 5647–57. doi:10.2174/092986712803988811. PMID 22856655.
- ^ a b c d "Coca Cultivation in the Andean Region" (PDF). UNODC. June 2006.
- ^ a b c Latorre F, Klimek L (January 1999). "Does cocaine still have a role in nasal surgery?". Drug Safety. 20 (1): 9–13. doi:10.2165/00002018-199920010-00002. PMID 9935273. S2CID 40598106.
- ^ a b c Armbuster YC, Banas BN, Feickert KD, England SE, Moyer EJ, Christie EL, et al. (December 2021). "Decline and Pronounced Regional Disparities in Medical Cocaine Usage in the United States". The Journal of Pharmacy Technology. 37 (6): 278–285. doi:10.1177/87551225211035563. PMC 8592245. PMID 34790964.
- ^ "Cocaine & Crack". Erowid.
- ^ a b "Cocaine". DEA.
- ^ Cortés E, Metaal P. Smokable cocaine markets in Latin America and the Caribbean (PDF).
- ^ a b Cheng MH, Block E, Hu F, Cobanoglu MC, Sorkin A, Bahar I (2015). "Insights into the Modulation of Dopamine Transporter Function by Amphetamine, Orphenadrine, and Cocaine Binding". Frontiers in Neurology. 6: 134. doi:10.3389/fneur.2015.00134. PMC 4460958. PMID 26106364.
- ^ Connors NJ, Hoffman RS (2013). "Cocaine toxicity". J Pharmacol Exp Ther. 347 (2): 251–257. doi:10.1124/jpet.113.206383. PMID 23978563.
- ^ Sordo L, Indave BI, Barrio G, Degenhardt L, de la Fuente L, Bravo MJ (September 2014). "Cocaine use and risk of stroke: a systematic review". Drug and Alcohol Dependence. 142: 1–13. doi:10.1016/j.drugalcdep.2014.06.041. PMID 25066468.
- ^ a b c Nitro L, Pipolo C, Fadda GL, Allevi F, Borgione M, Cavallo G, et al. (July 2022). "Distribution of cocaine-induced midline destructive lesions: systematic review and classification". European Archives of Oto-Rhino-Laryngology. 279 (7): 3257–3267. doi:10.1007/s00405-022-07290-1. PMC 9130192. PMID 35138441.
- ^ a b c Di Cosola M, Ambrosino M, Limongelli L, Favia G, Santarelli A, Cortelazzi R, et al. (July 2021). "Cocaine-Induced Midline Destructive Lesions (CIMDL): A Real Challenge in Diagnosis". International Journal of Environmental Research and Public Health. 18 (15): 7831. doi:10.3390/ijerph18157831. PMC 8345435. PMID 34360121.
- ^ a b Kohnen-Johannsen KL, Kayser O (February 2019). "Tropane Alkaloids: Chemistry, Pharmacology, Biosynthesis and Production". Molecules. 24 (4): 796. doi:10.3390/molecules24040796. PMC 6412926. PMID 30813289.
- ^ Busnel R, Manrique López H (July 2023). "The political economy of a failed drug reform: Insights from Peru's main legal coca valley". The International Journal on Drug Policy. 117: 104050. doi:10.1016/j.drugpo.2023.104050. PMID 37267739.
- ^ Grisaffi T, Ledebur K (31 March 2016). "Citizenship or Repression? Coca, Eradication and Development in the Andes". Stability: International Journal of Security and Development. 5 (1). doi:10.5334/sta.440. ISSN 2165-2627.
- ^ Housego K (5 April 2004). "As addiction rises, Colombia weighs rolling back decade-old drug legalization". The San Diego Union-Tribune. Associated Press. Retrieved 9 August 2009.
- ^ Murphy J (5 April 2004). "Colombia sinks in sea of legal cocaine, heroin". CBS News. Archived from the original on 5 April 2004. Retrieved 9 August 2009.
- ^ "Heroin and cocaine now legal in Mexico – in small doses | Americas | News | The Independent". The Independent. 23 October 2011. Retrieved 15 May 2016.
- ^ Greenwald G, Reuter P, Lynch T (3 April 2009). "Lessons for Creating Fair and Successful Drug Policies" (PDF). Drug Decriminalization in Portugal. Cato Institute.
- ^ a b Goldstein RA, DesLauriers C, Burda AM (January 2009). "Cocaine: history, social implications, and toxicity--a review". Disease-a-Month. 55 (1): 6–38. doi:10.1016/j.disamonth.2008.10.002. PMID 19081448.
- ^ Valdez LM, Taboada J, Valdez JE (June 2015). "Ancient Use of Coca Leaves in the Peruvian Central Highlands". Journal of Anthropological Research. 71 (2): 231–258. doi:10.3998/jar.0521004.0071.204. hdl:2027/spo.0521004.0071.204. S2CID 163842955.
- ^ Martin RT (October 1970). "The role of coca in the history, religion, and medicine of South American Indians". Economic Botany. 24 (4): 422–438. Bibcode:1970EcBot..24..422M. doi:10.1007/BF02860746. S2CID 34523519.
- ^ Plant T, Aref-Adib G (June 2008). "Travelling to new heights: practical high altitude medicine". British Journal of Hospital Medicine. 69 (6): 348–352. doi:10.12968/hmed.2008.69.6.29626. PMID 18646420.
- ^ Andrew M. Luks, et al. "Wilderness Medical Society Consensus Guidelines for the Prevention and Treatment of Acute Altitude Illness: 2014 Update". Wilderness & Environmental Medicine, 25, S4–S14 (2014).
- ^ World Drug Report 2021: Booklet 4 (PDF). [S.l.]: United Nations Office on Drugs and Crime. 2021. p. 35. ISBN 978-92-1-148361-1. Archived (PDF) from the original on 24 June 2021.
- ^ Room R, Reuter P (January 2012). "How well do international drug conventions protect public health?". Lancet. 379 (9810): 84–91. doi:10.1016/s0140-6736(11)61423-2. PMID 22225673. S2CID 23386203.
The international treaties have also constrained national policy experimentation because they require nation states to criminalise drug use
- ^ "Drug Fact Sheet: Cocaine" (PDF). Drug Enforcement Agency. Archived (PDF) from the original on 21 June 2020. Retrieved 17 June 2022.
- ^ "Drug Fact Sheet: Cocaine" (PDF). US Department for Justice and Drug Enforcement Administration. Archived (PDF) from the original on 21 June 2020. Retrieved 29 June 2024.
- ^ "The tradition of chewing coca". 15 August 2013. Archived from the original on 6 May 2021. Retrieved 6 May 2021.
- ^ Embury-Dennis T. "It's legal to manufacture cocaine and heroin for medical use — and Britain is the world's biggest exporter". Business Insider. Archived from the original on 28 July 2020. Retrieved 17 March 2019.
- ^ "Cocaine: Effects, Hazards & Warnings". Drugs.com. Archived from the original on 28 July 2020. Retrieved 17 March 2019.
- ^ Siegel RK, Elsohly MA, Plowman T, Rury PM, Jones RT (January 1986). "Cocaine in herbal tea". JAMA. 255 (1): 40. doi:10.1001/jama.1986.03370010042021. PMID 3940302.
- ^ Schultes RE (1957). "A New Method of Coca Preparation in the Colombian Amazon". Botanical Museum Leaflets, Harvard University. 17 (9): 241–246. doi:10.5962/p.168505. ISSN 0006-8098. JSTOR 41762172.
- ^ Dwyer C, Sowerby L, Rotenberg BW (August 2016). "Is cocaine a safe topical agent for use during endoscopic sinus surgery?". The Laryngoscope (Review). 126 (8): 1721–1723. doi:10.1002/lary.25836. PMID 27075241.
- ^ Benjamin E, Wong DK, Choa D (December 2004). "'Moffett's' solution: a review of the evidence and scientific basis for the topical preparation of the nose". Clinical Otolaryngology and Allied Sciences. 29 (6): 582–587. doi:10.1111/j.1365-2273.2004.00894.x. PMID 15533141.
- ^ Hamdan AL, Sataloff RT, Hawkshaw MJ (2022). "Topical Anesthesia in Office-Based Laryngeal Surgery". Office-Based Laryngeal Surgery. USA: Springer. pp. 123–137. doi:10.1007/978-3-030-91936-8_6. ISBN 978-3-030-91935-1. Archived from the original on 18 July 2022. Retrieved 18 July 2022.
- ^ "Drug Approval Package: Goprelto (cocaine hydrochloride)". U.S. Food and Drug Administration (FDA). 30 April 2018. Archived from the original on 28 July 2020. Retrieved 30 April 2020.
- ^
 This article incorporates text from this source, which is in the public domain: "Numbrino: FDA-Approved Drugs". U.S. Food and Drug Administration (FDA). Archived from the original on 28 July 2020. Retrieved 30 April 2020.
This article incorporates text from this source, which is in the public domain: "Numbrino: FDA-Approved Drugs". U.S. Food and Drug Administration (FDA). Archived from the original on 28 July 2020. Retrieved 30 April 2020.
- ^ Berkowitz AL (2022). "Chapter 10: Pupillary Control & Approach to Anisocoria: Cranial Nerves 2 & 3". Clinical Neurology & Neuroanatomy: A Localization-Based Approach (Digital) (2nd ed.). McGraw Hill. ISBN 978-1260453362.
- ^ a b World Health Organization (2004). Neuroscience of psychoactive substance use and dependence. World Health Organization. p. 89. ISBN 978-9241562355. Archived from the original on 30 April 2016.
- ^ World Health Organization (2007). International medical guide for ships. World Health Organization. p. 242. ISBN 978-9241547208. Archived from the original on 30 April 2016.
- ^ a b Sordo L, Indave BI, Barrio G, Degenhardt L, de la Fuente L, Bravo MJ (September 2014). "Cocaine use and risk of stroke: a systematic review". Drug and Alcohol Dependence (Systematic Review). 142: 1–13. doi:10.1016/j.drugalcdep.2014.06.041. PMID 25066468.
- ^ Donroe JH, Tetrault JM (July 2017). "Substance Use, Intoxication, and Withdrawal in the Critical Care Setting". Critical Care Clinics (Review). 33 (3): 543–558. doi:10.1016/j.ccc.2017.03.003. PMID 28601134.
- ^ Fehrman E, Egan V, Gorban AN, Levesley J, Mirkes EM, Muhammad AK (2019). Personality Traits and Drug Consumption. A Story Told by Data. Springer, Cham. arXiv:2001.06520. doi:10.1007/978-3-030-10442-9. ISBN 978-3-030-10441-2. S2CID 151160405.
- ^ "Patients face losing noses due to cocaine use, medics warn". 9 March 2023.
- ^ Veevers L (1 October 2006). "'Shared banknote' health warning to cocaine users". The Observer. Retrieved 26 July 2008.
- ^ "DrugFacts: Cocaine". National Institute on Drug Abuse. April 2013. Archived from the original on 11 July 2015. Retrieved 11 July 2015.
- ^ "The Dangers Of Snorting Cocaine (Insufflation)". Vertava Health. Archived from the original on 8 April 2022. Retrieved 25 February 2022.
- ^ a b Volkow ND, Wang GJ, Fischman MW, Foltin R, Fowler JS, Franceschi D, et al. (August 2000). "Effects of route of administration on cocaine-induced dopamine transporter blockade in the human brain". Life Sciences. 67 (12): 1507–1515. doi:10.1016/S0024-3205(00)00731-1. PMID 10983846.
- ^ "Drug Money". Snopes. 9 July 2002. Retrieved 23 July 2008.
- ^ Abrahamson A (13 November 1994). "Prevalence of Drug-Tainted Money Voids Case Law: Court cites findings that more than 75% of currency in L.A. bears traces of cocaine or other illegal substances". Los Angeles Times. Archived from the original on 4 June 2011. Retrieved 23 July 2008.
- ^ Price DM (6 May 1990). "Use of Drug-Sniffing Dogs Challenged;ACLU Backs Complaint by Men Whose Pocket Cash Was Seized". The Washington Post. Archived from the original on 4 June 2011. Retrieved 23 July 2008.
- ^ "Sniffing Around the History of the McDonald's 'Cocaine Spoon'". www.mentalfloss.com. 19 March 2021. Archived from the original on 8 July 2024. Retrieved 14 June 2021.
- ^ "Cocaine terminology". Archived from the original on 9 July 2007.
- ^ Bonkovsky HL, Mehta S (February 2001). "Hepatitis C: a review and update". Journal of the American Academy of Dermatology. 44 (2): 159–182. doi:10.1067/mjd.2001.109311. PMID 11174373.
- ^ "Code of ordinances village of Dundee, Michigan. Chapter 51". Village of Dundee.
- ^ "Code of Ordinances – Clark County, NV". Municode Library. Archived from the original on 13 September 2024. Retrieved 13 September 2024.
- ^ "Township of Middlesex, PA Drugs and Drug Paraphernalia". eCode360. Archived from the original on 13 September 2024. Retrieved 13 September 2024.
- ^ Graybosch AJ (1 January 2004). "American Beauty". Deconstruction and Reconstruction. Brill. p. 96. doi:10.1163/9789004495876_013. ISBN 978-90-420-1681-1.
- ^ Ries RK, Miller SC, Fiellin DA (2009). Principles of addiction medicine. Lippincott Williams & Wilkins. p. 137. ISBN 978-0-7817-7477-2. Archived from the original on 4 April 2014. Retrieved 5 January 2014.
- ^ a b Richards JR, Laurin EG (June 2023). "Cocaine". StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. PMID 28613520.
- ^ a b c d "Cocaine as a Teratogen". Embryo Project Encyclopedia. Arizona State University. Retrieved 7 April 2025.
- ^ Singer L, Arendt R, Minnes S (March 1993). "Neurodevelopmental effects of cocaine". Clinics in Perinatology. 20 (1): 245–262. doi:10.1016/S0095-5108(18)30422-6. PMC 4181371. PMID 8458168.
- ^ Cain MA, Bornick P, Whiteman V (March 2013). "The maternal, fetal, and neonatal effects of cocaine exposure in pregnancy". Clinical Obstetrics and Gynecology. 56 (1): 124–132. doi:10.1097/GRF.0b013e31827ae167. PMID 23314714.
- ^ Flowers D, Clark JF, Westney LS (March 1991). "Cocaine intoxication associated with abruptio placentae". Journal of the National Medical Association. 83 (3): 230–232. PMC 2627035. PMID 2038082.
- ^ "When breastfeeding or feeding expressed milk is not recommended". Centers for Disease Control and Prevention. 10 August 2021. Retrieved 14 November 2021.
- ^ Eglash A, Leeper K (2020). The Little Green Book of Breastfeeding Management for Physicians & Other Healthcare Providers (7 ed.). Madison, WI: The Institute for the Advancement of Breastfeeding and Lactation Education. ISBN 978-0-9987789-0-7.
- ^ "Street Drugs and pregnancy". March of Dimes. Archived from the original on 5 September 2015. Retrieved 26 May 2009.
- ^ Nutt DJ, King LA, Phillips LD (November 2010). "Drug harms in the UK: a multicriteria decision analysis". Lancet. 376 (9752): 1558–65. CiteSeerX 10.1.1.690.1283. doi:10.1016/S0140-6736(10)61462-6. PMID 21036393. S2CID 5667719.
- ^ Nutt D, King LA, Saulsbury W, Blakemore C (March 2007). "Development of a rational scale to assess the harm of drugs of potential misuse". Lancet. 369 (9566): 1047–53. doi:10.1016/S0140-6736(07)60464-4. PMID 17382831. S2CID 5903121.
- ^ Talarico GP, Crosta ML, Giannico MB, Summaria F, Calò L, Patrizi R (May 2017). "Cocaine and coronary artery diseases: a systematic review of the literature". Journal of Cardiovascular Medicine. 18 (5): 291–294. doi:10.2459/JCM.0000000000000511. PMID 28306693.
- ^ a b c d "2017 National Drug Threat Assessment" (PDF). Drug Enforcement Administration. 1 October 2017. Retrieved 17 June 2025.
- ^ Fredericks C, Yon JR, Alex G, Morton M, Messer T, Bokhari F, et al. (March 2017). "Levamisole-induced Necrosis Syndrome: Presentation and Management". Wounds. 29 (3): 71–76. PMID 28355139.
- ^ Morris GW, Mason BC, Harris Sprunger R, Hake Harris H, White LA, Patterson DA (2012). "Levamisole-adulterated cocaine: a case series". Journal of the American Board of Family Medicine. 25 (4): 531–535. doi:10.3122/jabfm.2012.04.110287. PMID 22773722.
- ^ Lee KC, Ladizinski B, Federman DG (June 2012). "Complications associated with use of levamisole-contaminated cocaine: an emerging public health challenge". Mayo Clinic Proceedings. 87 (6): 581–586. doi:10.1016/j.mayocp.2012.03.010. PMC 3498128. PMID 22677078.
- ^ "Cocaine retail markets: multiple indicators suggest continued growth and diversification | www.euda.europa.eu". www.euda.europa.eu.
- ^ Chang A, Osterloh J, Thomas J (September 2010). "Levamisole: a dangerous new cocaine adulterant". Clinical Pharmacology and Therapeutics. 88 (3): 408–411. doi:10.1038/clpt.2010.156. PMID 20668440. S2CID 31414939.
- ^ Tallarida CS, Egan E, Alejo GD, Raffa R, Tallarida RJ, Rawls SM (April 2014). "Levamisole and cocaine synergism: a prevalent adulterant enhances cocaine's action in vivo". Neuropharmacology. 79: 590–595. doi:10.1016/j.neuropharm.2014.01.002. PMC 3989204. PMID 24440755.
- ^ Chang A, Osterloh J, Thomas J (September 2010). "Levamisole: a dangerous new cocaine adulterant". Clinical Pharmacology and Therapeutics. 88 (3): 408–411. doi:10.1038/clpt.2010.156. PMID 20668440. S2CID 31414939.
- ^ Gill H, Trinh D, Anderson DJ, Li N, Madenberg D (August 2021). "Cocaine and Levamisole Induced Vasculitis". Cureus. 13 (8): e17192. doi:10.7759/cureus.17192. PMC 8439268. PMID 34548986.
- ^ Iorio L, Davanzo F, Cazzador D, Codirenzi M, Fiorin E, Zanatta E, et al. (August 2024). "Cocaine- and Levamisole-Induced Vasculitis: Defining the Spectrum of Autoimmune Manifestations". Journal of Clinical Medicine. 13 (17): 5116. doi:10.3390/jcm13175116. PMC 11396482. PMID 39274328.
- ^ Cascio MJ, Jen KY (January 2018). "Cocaine/levamisole-associated autoimmune syndrome: a disease of neutrophil-mediated autoimmunity". Current Opinion in Hematology. 25 (1): 29–36. doi:10.1097/MOH.0000000000000393. PMID 29211697.
- ^ Cascio MJ, Jen KY (January 2018). "Cocaine/levamisole-associated autoimmune syndrome: a disease of neutrophil-mediated autoimmunity". Current Opinion in Hematology. 25 (1): 29–36. doi:10.1097/MOH.0000000000000393. PMID 29211697. S2CID 23795272.
- ^ Peacock A, Tran LT, Larney S, Stockings E, Santo T, Jones H, et al. (April 2021). "All-cause and cause-specific mortality among people with regular or problematic cocaine use: a systematic review and meta-analysis". Addiction. 116 (4): 725–742. doi:10.1111/add.15239. PMC 7914269. PMID 32857457.
- ^ "Cocaine or alcohol, what's worse?". Liberty House Clinic. 17 February 2025. Retrieved 19 April 2025.
- ^ a b Clare K, Park K, Pan Y, Lejuez CW, Volkow ND, Du C (2024). "Neurovascular effects of cocaine: relevance to addiction". Frontiers in Pharmacology. 15: 1357422. doi:10.3389/fphar.2024.1357422. PMC 10917943. PMID 38455961.
- ^ Nicolucci C, Pais ML, Santos AC, Ribeiro FM, Encarnação PM, Silva AL, et al. (2020). "Single Low Dose of Cocaine-Structural Brain Injury Without Metabolic and Behavioral Changes". Frontiers in Neuroscience. 14: 589897. doi:10.3389/fnins.2020.589897. PMC 7874143. PMID 33584173.
- ^ Hofmaier T, Luf A, Seddik A, Stockner T, Holy M, Freissmuth M, et al. (July 2014). "Aminorex, a metabolite of the cocaine adulterant levamisole, exerts amphetamine like actions at monoamine transporters". Neurochemistry International. 73 (100): 32–41. doi:10.1016/j.neuint.2013.11.010. PMC 4077236. PMID 24296074.
- ^ Brady KT, Lydiard RB, Malcolm R, Ballenger JC (December 1991). "Cocaine-induced psychosis". The Journal of Clinical Psychiatry. 52 (12): 509–512. PMID 1752853.
- ^ a b c Thirthalli J, Benegal V (May 2006). "Psychosis among substance users". Current Opinion in Psychiatry. 19 (3): 239–245. doi:10.1097/01.yco.0000218593.08313.fd. PMID 16612208. S2CID 13350537.
- ^ Elliott A, Mahmood T, Smalligan RD (2012). "Cocaine bugs: a case report of cocaine-induced delusions of parasitosis". The American Journal on Addictions. 21 (2): 180–181. doi:10.1111/j.1521-0391.2011.00208.x. PMID 22332864.
- ^ DiSclafani II A, Hall RC, Gardner ER (October 1981). "Drug-induced psychosis: emergency diagnosis and management". Psychosomatics. 22 (10): 845–50, 855. doi:10.1016/s0033-3182(81)73092-5. PMID 7313045.
- ^ Heesch CM, Negus BH, Keffer JH, Snyder RW, Risser RC, Eichhorn EJ (August 1995). "Effects of cocaine on cortisol secretion in humans". The American Journal of the Medical Sciences. 310 (2): 61–4. doi:10.1097/00000441-199508000-00004. PMID 7631644. S2CID 11042810.
- ^ a b Ambre JJ, Belknap SM, Nelson J, Ruo TI, Shin SG, Atkinson AJ (July 1988). "Acute tolerance to cocaine in humans". Clinical Pharmacology and Therapeutics. 44 (1): 1–8. doi:10.1038/clpt.1988.104. PMID 3390996. S2CID 44253676.
- ^ Pudiak CM, KuoLee R, Bozarth MA (July 2014). "Tolerance to cocaine in brain stimulation reward following continuous cocaine infusions". Pharmacology, Biochemistry, and Behavior. 122: 246–52. doi:10.1016/j.pbb.2014.04.006. PMID 24768900. S2CID 207332822.
- ^ Gullapalli BT, Natarajan A, Angarita GA, Malison RT, Ganesan D, Rahman T (21 June 2019). "On-body Sensing of Cocaine Craving, Euphoria and Drug-Seeking Behavior Using Cardiac and Respiratory Signals". Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies. 3 (2): 1–31. doi:10.1145/3328917. S2CID 195357215.
- ^ Calipari ES, Ferris MJ, Jones SR (January 2014). "Extended access of cocaine self-administration results in tolerance to the dopamine-elevating and locomotor-stimulating effects of cocaine". Journal of Neurochemistry. 128 (2): 224–32. doi:10.1111/jnc.12452. PMC 3947316. PMID 24102293.
- ^ a b Zhao W (2008). Mechanisms Mediating Sex Differences in the Effects of Cocaine. University of Michigan. p. 3. ISBN 978-0-549-99458-9. Archived from the original on 4 April 2014. Retrieved 25 September 2012.
- ^ Boles SM, Miotto K (March–April 2003). "Substance abuse and violence: A review of the literature". Aggression and Violent Behavior. 8 (2): 155–174. doi:10.1016/S1359-1789(01)00057-X.
- ^ Pergolizzi JV, Magnusson P, LeQuang JA, Breve F, Varrassi G (April 2021). "Cocaine and Cardiotoxicity: A Literature Review". Cureus. 13 (4): e14594. doi:10.7759/cureus.14594. ISSN 2168-8184. PMC 8136464. PMID 34036012.
- ^ a b Treadwell SD, Robinson TG (June 2007). "Cocaine use and stroke". Postgraduate Medical Journal. 83 (980): 389–394. doi:10.1136/pgmj.2006.055970. PMC 2600058. PMID 17551070.
- ^ Havakuk O, Rezkalla SH, Kloner RA (July 2017). "The Cardiovascular Effects of Cocaine". Journal of the American College of Cardiology (Review). 70 (1): 101–113. doi:10.1016/j.jacc.2017.05.014. PMID 28662796.
- ^ Frazer KM, Richards Q, Keith DR (August 2018). "The long-term effects of cocaine use on cognitive functioning: A systematic critical review". Behavioural Brain Research. 348: 241–262. doi:10.1016/j.bbr.2018.04.005. PMID 29673580. S2CID 4992738.
- ^ D'haenen H, den Boer JA, Willner P, eds. (2002). Biological Psychiatry. Vol. 2 (2 ed.). Wiley. p. 528. ISBN 978-0-471-49198-9.
- ^ Wang GJ, Volkow ND, Fowler JS, Fischman M, Foltin R, Abumrad NN, et al. (8 August 1997). "Cocaine abusers do not show loss of dopamine transporters with age". Life Sciences. 61 (11): 1059–65. doi:10.1016/s0024-3205(97)00614-0. PMID 9307051.
- ^ Little KY, Ramssen E, Welchko R, Volberg V, Roland CJ, Cassin B (August 2009). "Decreased brain dopamine cell numbers in human cocaine users". Psychiatry Research. 168 (3): 173–80. doi:10.1016/j.psychres.2008.10.034. PMID 19233481. S2CID 27618292.
- ^ Sharma HS, Muresanu D, Sharma A, Patnaik R (2009). "Cocaine-induced breakdown of the blood–brain barrier and neurotoxicity". International Review of Neurobiology. 88: 297–334. doi:10.1016/S0074-7742(09)88011-2. ISBN 978-0-12-374504-0. PMID 19897082.
- ^ Karch SB (2009). Karch's pathology of drug abuse (4 ed.). Boca Raton: CRC Press. p. 70. ISBN 978-0-8493-7881-2. Archived from the original on 10 September 2017.
- ^ Vijayakumar L, Kumar MS, Vijayakumar V (May 2011). "Substance use and suicide". Current Opinion in Psychiatry. 24 (3): 197–202. doi:10.1097/YCO.0b013e3283459242. PMID 21430536. S2CID 206143129.
- ^ Moçambique M, Hoffmann A, Roglio V, Kessler F, Dalbosco C, Schuch J, et al. (24 June 2022). "Prevalence of suicide in cocaine users accessing health services: a systematic review and meta-analysis". Revista Brasileira de Psiquiatria. 44 (4). Sao Paulo, Brazil: 441–448. doi:10.47626/1516-4446-2021-2207. PMC 9375660. PMID 35751594.
- ^ Ayd FJ (2000). Lexicon of psychiatry, neurology, and the neurosciences (2nd ed.). Philadelphia [u.a.]: Lippincott Williams & Wilkins. p. 256. ISBN 978-0-7817-2468-5.
- ^ Shekarchizadeh H, Khami MR, Mohebbi SZ, Ekhtiari H, Virtanen JI (September 2013). "Oral Health of Drug Abusers: A Review of Health Effects and Care". Iranian Journal of Public Health. 42 (9): 929–940. PMC 4453891. PMID 26060654.
- ^ Baigent M (2003). "Physical complications of substance abuse: what the psychiatrist needs to know". Curr Opin Psychiatry. 16 (3): 291–296. doi:10.1097/00001504-200305000-00004.
- ^ "Cocaine". NIDA.
- ^ Paludetto LS, Florence LL, Torales J, Ventriglio A, Castaldelli-Maia JM (29 March 2024). "Mapping the Neural Substrates of Cocaine Craving: A Systematic Review". Brain Sciences. 14 (4): 329. doi:10.3390/brainsci14040329. PMC 11048489. PMID 38671981.
- ^ Walsh SL, Stoops WW, Moody DE, Lin SN, Bigelow GE (August 2009). "Repeated dosing with oral cocaine in humans: assessment of direct effects, withdrawal, and pharmacokinetics". Experimental and Clinical Psychopharmacology. 17 (4): 205–216. doi:10.1037/a0016469. PMC 2811070. PMID 19653786.
- ^ "Fentanyl-Adulterated Cocaine: Strategies To Address The New Normal". 25 April 2019. Archived from the original on 17 December 2022. Retrieved 17 December 2022.
- ^ Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. (GBD 2017 Causes of Death Collaborators) (November 2018). "Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017". Lancet. 392 (10159): 1736–1788. doi:10.1016/S0140-6736(18)32203-7. PMC 6227606. PMID 30496103.
- ^ Hampton WH, Hanik I, Olson IR (2019). "[Substance Abuse and White Matter: Findings, Limitations, and Future of Diffusion Tensor Imaging Research]". Drug and Alcohol Dependence. 197 (4): 288–298. doi:10.1016/j.drugalcdep.2019.02.005. PMC 6440853. PMID 30875650.
- ^ Fernàndez-Castillo N, Cabana-Domínguez J, Corominas R, Cormand B (January 2022). "Molecular genetics of cocaine use disorders in humans". Molecular Psychiatry. 27 (1): 624–639. doi:10.1038/s41380-021-01256-1. PMC 8960411. PMID 34453125.
- ^ Hope BT (May 1998). "Cocaine and the AP-1 transcription factor complex". Annals of the New York Academy of Sciences. 844 (1): 1–6. Bibcode:1998NYASA.844....1H. doi:10.1111/j.1749-6632.1998.tb08216.x. PMID 9668659. S2CID 11683570. Archived from the original on 28 July 2020. Retrieved 30 June 2019.
- ^ a b Kelz MB, Chen J, Carlezon WA, Whisler K, Gilden L, Beckmann AM, et al. (September 1999). "Expression of the transcription factor deltaFosB in the brain controls sensitivity to cocaine". Nature. 401 (6750): 272–6. Bibcode:1999Natur.401..272K. doi:10.1038/45790. PMID 10499584. S2CID 4390717.
- ^ Colby CR, Whisler K, Steffen C, Nestler EJ, Self DW (March 2003). "Striatal cell type-specific overexpression of DeltaFosB enhances incentive for cocaine". The Journal of Neuroscience. 23 (6): 2488–93. doi:10.1523/JNEUROSCI.23-06-02488.2003. PMC 6742034. PMID 12657709.
- ^ a b Nestler EJ, Barrot M, Self DW (September 2001). "DeltaFosB: a sustained molecular switch for addiction". Proceedings of the National Academy of Sciences of the United States of America. 98 (20): 11042–6. Bibcode:2001PNAS...9811042N. doi:10.1073/pnas.191352698. PMC 58680. PMID 11572966.
- ^ de Souza MF, Gonçales TA, Steinmetz A, Moura DJ, Saffi J, Gomez R, et al. (April 2014). "Cocaine induces DNA damage in distinct brain areas of female rats under different hormonal conditions". Clinical and Experimental Pharmacology & Physiology. 41 (4): 265–9. doi:10.1111/1440-1681.12218. PMID 24552452. S2CID 20849951.
- ^ Alvarenga TA, Andersen ML, Ribeiro DA, Araujo P, Hirotsu C, Costa JL, et al. (January 2010). "Single exposure to cocaine or ecstasy induces DNA damage in brain and other organs of mice". Addiction Biology. 15 (1): 96–9. doi:10.1111/j.1369-1600.2009.00179.x. PMID 19878142. S2CID 21347765.
- ^ Dabin J, Fortuny A, Polo SE (June 2016). "Epigenome Maintenance in Response to DNA Damage". Molecular Cell. 62 (5): 712–27. doi:10.1016/j.molcel.2016.04.006. PMC 5476208. PMID 27259203.
- ^ Gawin FH, Ellinwood EH (1989). "Cocaine dependence". Annual Review of Medicine. 40: 149–61. doi:10.1146/annurev.me.40.020189.001053. PMID 2658744.
- ^ Sofuoglu M, Dudish-Poulsen S, Poling J, Mooney M, Hatsukami DK (July 2005). "The effect of individual cocaine withdrawal symptoms on outcomes in cocaine users". Addictive Behaviors. 30 (6): 1125–1134. doi:10.1016/j.addbeh.2004.10.010. PMID 15925122.
- ^ a b Kampman KM (October 2019). "The treatment of cocaine use disorder". Science Advances. 5 (10): eaax1532. Bibcode:2019SciA....5.1532K. doi:10.1126/sciadv.aax1532. PMC 6795516. PMID 31663022.
- ^ Cocaine Anonymous (13 November 2007). "And All Other Mind-Altering Substances". Archived from the original on 4 March 2009. Retrieved 15 November 2007.
- ^ Minozzi S, Cinquini M, Amato L, Davoli M, Farrell MF, Pani PP, et al. (April 2015). Minozzi S (ed.). "Anticonvulsants for cocaine dependence". The Cochrane Database of Systematic Reviews (Systematic Review & Meta-Analysis). 2015 (4): CD006754. doi:10.1002/14651858.CD006754.pub4. PMC 8812341. PMID 25882271.
- ^ McClure EA, Gipson CD, Malcolm RJ, Kalivas PW, Gray KM (2014). "Potential role of N-acetylcysteine in the management of substance use disorders". CNS Drugs. 28 (2): 95–106. doi:10.1007/s40263-014-0142-x. PMC 4009342. PMID 24442756.
- ^ Berberi A, Azar E (2024). "Oral Rehabilitation for a Patient with Cocaine-Induced Midline Destructive Lesions". Case Reports in Otolaryngology. 2024: 7109261. doi:10.1155/2024/7109261. PMC 11208820. PMID 38939732.
- ^ Jalali A (October 2023). "Cocaine Nose Correction: A Nonsurgical Approach Using a Novel Hyaluronic Acid Filler". Plastic and Reconstructive Surgery. Global Open. 11 (10): e5329. doi:10.1097/GOX.0000000000005329. PMC 10561808. PMID 37817926.
- ^ Taams KO, Taams SJ (January 2022). "The Bilateral Trans Alar Forehead Flap to Reconstruct the Cocaine Nose: A Case Report". Plastic and Reconstructive Surgery. Global Open. 10 (1): e4044. doi:10.1097/GOX.0000000000004044. PMC 8785930. PMID 35083102.
- ^ Chatzaraki V, Schweitzer W, Thali MJ, Ampanozi G (September 2019). "Nasal Septum Defects Detected on Postmortem Computed Tomography". The American Journal of Forensic Medicine and Pathology. 40 (3): 279–284. doi:10.1097/PAF.0000000000000482. PMID 30985333.
- ^ Schwartz R, Estroff T, Fairbanks D, Hoffmann N (January 1989). "Nasal symptoms associated with cocaine abuse during adolescence". Archives of Otolaryngology--head & Neck Surgery. 115 (1): 63–64. doi:10.1001/archotol.1989.01860250065028. PMID 2909232.
- ^ a b "Fraser 'Nose' The Irreparable Damage Cocaine Use Can Do | NHS Lanarkshire". www.nhslanarkshire.scot.nhs.uk.
- ^ a b "Patients face losing noses due to cocaine use, medics warn". 9 March 2023.
- ^ Schreiber BE, Twigg S, Marais J, Keat AC (April–May 2014). "Saddle-nose deformities in the rheumatology clinic". Ear, Nose, & Throat Journal (Review). 93 (4–5): E45 – E47. PMID 24817241.
- ^ a b Pagliaro L, Pagliaro AM (2004). Pagliaros' Comprehensive Guide to Drugs and Substances of Abuse. Washington, D.C.: American Pharmacists Association. ISBN 978-1-58212-066-9.
- ^ Hansen FV, Kiehn OT, Lomholt AF, Ringdom H, Aanæs K (October 2023). "[Not Available]". Ugeskrift for Laeger. 185 (40). PMID 37874002.
- ^ Millard DR, Mejia FA (February 2001). "Reconstruction of the nose damaged by cocaine". Plastic and Reconstructive Surgery. 107 (2): 419–424. doi:10.1097/00006534-200102000-00018. PMID 11214057.
- ^ "Doctors in Belgium see serious nose lesions amid rising cocaine use". euronews. 28 March 2024.
- ^ Overdose Death Rates. By National Institute on Drug Abuse (NIDA).
- ^ O'Leary ME, Hancox JC (May 2010). "Role of voltage-gated sodium, potassium and calcium channels in the development of cocaine-associated cardiac arrhythmias". British Journal of Clinical Pharmacology. 69 (5): 427–442. doi:10.1111/j.1365-2125.2010.03629.x. PMC 2856043. PMID 20573078.
- ^ "Cocaine". LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases. 2017. PMID 31643773.
- ^ "Cocaine use fuels record high in drug deaths". www.bbc.com. 23 October 2024.
- ^ Laizure SC, Mandrell T, Gades NM, Parker RB (January 2003). "Cocaethylene metabolism and interaction with cocaine and ethanol: role of carboxylesterases". Drug Metabolism and Disposition. 31 (1): 16–20. doi:10.1124/dmd.31.1.16. PMID 12485948.
- ^ Pergolizzi J, Breve F, Magnusson P, LeQuang JA, Varrassi G (February 2022). "Cocaethylene: When Cocaine and Alcohol Are Taken Together". Cureus. 14 (2): e22498. doi:10.7759/cureus.22498. PMC 8956485. PMID 35345678.
- ^ Liu X, Singer ME (June 2023). "Intentional use of both opioids and cocaine in the United States". Preventive Medicine Reports. 33: 102227. doi:10.1016/j.pmedr.2023.102227. PMC 10201855. PMID 37223567.
- ^ Barnett G, Hawks R, Resnick R (1981). "Cocaine pharmacokinetics in humans". Journal of Ethnopharmacology. 3 (2–3): 353–66. doi:10.1016/0378-8741(81)90063-5. PMID 7242115.; Jones, supra note 19; Wilkinson et al., Van Dyke et al.
- ^ Sachkova A, Doetsch DA, Jensen O, Brockmöller J, Ansari S (October 2021). "How do psychostimulants enter the human brain? Analysis of the role of the proton-organic cation antiporter". Biochemical Pharmacology. 192: 114751. doi:10.1016/j.bcp.2021.114751. PMID 34464621.
- ^ Tega Y, Tabata H, Kurosawa T, Kitamura A, Itagaki F, Oshitari T, et al. (January 2021). "Structural Requirements for Uptake of Diphenhydramine Analogs into hCMEC/D3 Cells Via the Proton-Coupled Organic Cation Antiporter". Journal of Pharmaceutical Sciences. 110 (1): 397–403. doi:10.1016/j.xphs.2020.09.001. PMID 32898521.
- ^ Chapy H, Smirnova M, André P, Schlatter J, Chiadmi F, Couraud PO, et al. (October 2014). "Carrier-mediated cocaine transport at the blood–brain barrier as a putative mechanism in addiction liability". The International Journal of Neuropsychopharmacology. 18 (1): pyu001. doi:10.1093/ijnp/pyu001. PMC 4368859. PMID 25539501.
- ^ Sachkova A, Jensen O, Dücker C, Ansari S, Brockmöller J (September 2022). "The mystery of the human proton-organic cation antiporter: One transport protein or many?". Pharmacology & Therapeutics. 239: 108283. doi:10.1016/j.pharmthera.2022.108283. PMID 36162727. S2CID 252527522.
- ^ Ambre J, Ruo TI, Nelson J, Belknap S (November 1988). "Urinary excretion of cocaine, benzoylecgonine, and ecgonine methyl ester in humans". Journal of Analytical Toxicology. 12 (6): 301–6. doi:10.1093/jat/12.6.301. PMID 3244269.
- ^ Kolbrich EA, Barnes AJ, Gorelick DA, Boyd SJ, Cone EJ, Huestis MA (October 2006). "Major and minor metabolites of cocaine in human plasma following controlled subcutaneous cocaine administration". Journal of Analytical Toxicology. 30 (8): 501–10. doi:10.1093/jat/30.8.501. PMID 17132243. Archived from the original on 18 July 2012.
- ^ "Schaffer Library of Drug Policy: Urine Testing for Cocaine". Retrieved 3 April 2025.
- ^ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 9th edition, Biomedical Publications, Seal Beach, California, 2011, pp. 390–394.
- ^ Czykanski M (30 December 2015). "Cocaine Metabolites in Hair". Chemistry Views. Archived from the original on 22 July 2019. Retrieved 22 July 2019.
- ^ Proebstl L, Kamp F, Manz K, Krause D, Adorjan K, Pogarell O, et al. (June 2019). "Effects of stimulant drug use on the dopaminergic system: A systematic review and meta-analysis of in vivo neuroimaging studies". European Psychiatry. 59: 15–24. doi:10.1016/j.eurpsy.2019.03.003. PMID 30981746.
- ^ "How does cocaine produce its effects?". Archived from the original on 18 January 2022. Retrieved 12 May 2021.
- ^ Wise RA, Robble MA (January 2020). "Dopamine and Addiction". Annual Review of Psychology. 71 (1): 79–106. doi:10.1146/annurev-psych-010418-103337. PMID 31905114.
- ^ Rothman RB, Baumann MH, Dersch CM, Romero DV, Rice KC, Carroll FI, et al. (January 2001). "Amphetamine-type central nervous system stimulants release norepinephrine more potently than they release dopamine and serotonin". Synapse. 39 (1): 32–41. doi:10.1002/1098-2396(20010101)39:1<32::AID-SYN5>3.0.CO;2-3. PMID 11071707. S2CID 15573624. (Table V. on page 37)
- ^ Hummel M, Unterwald EM (April 2002). "D1 dopamine receptor: a putative neurochemical and behavioral link to cocaine action". Journal of Cellular Physiology. 191 (1): 17–27. doi:10.1002/jcp.10078. PMID 11920678. S2CID 40444893.
- ^ Carta M, Allan AM, Partridge LD, Valenzuela CF (January 2003). "Cocaine inhibits 5-HT3 receptor function in neurons from transgenic mice overexpressing the receptor". European Journal of Pharmacology. 459 (2–3): 167–9. doi:10.1016/S0014-2999(02)02867-4. PMID 12524142.
- ^ Filip M, Bubar MJ, Cunningham KA (September 2004). "Contribution of serotonin (5-hydroxytryptamine; 5-HT) 5-HT2 receptor subtypes to the hyperlocomotor effects of cocaine: acute and chronic pharmacological analyses". The Journal of Pharmacology and Experimental Therapeutics. 310 (3): 1246–54. doi:10.1124/jpet.104.068841. PMID 15131246. S2CID 25809734.
- ^ Beuming T, Kniazeff J, Bergmann ML, Shi L, Gracia L, Raniszewska K, et al. (July 2008). "The binding sites for cocaine and dopamine in the dopamine transporter overlap". Nature Neuroscience. 11 (7): 780–9. doi:10.1038/nn.2146. PMC 2692229. PMID 18568020.
- ^ Volkow ND, Wang GJ, Fischman MW, Foltin RW, Fowler JS, Abumrad NN, et al. (April 1997). "Relationship between subjective effects of cocaine and dopamine transporter occupancy". Nature. 386 (6627): 827–830. Bibcode:1997Natur.386..827V. doi:10.1038/386827a0. PMID 9126740.
- ^ a b Heal DJ, Gosden J, Smith SL (December 2014). "Dopamine reuptake transporter (DAT) "inverse agonism"--a novel hypothesis to explain the enigmatic pharmacology of cocaine". Neuropharmacology. CNS Stimulants. 87: 19–40. doi:10.1016/j.neuropharm.2014.06.012. PMID 24953830.
- ^ Volkow ND, Wang GJ, Fowler JS, Gatley SJ, Ding YS, Logan J, et al. (September 1996). "Relationship between psychostimulant-induced "high" and dopamine transporter occupancy". Proceedings of the National Academy of Sciences of the United States of America. 93 (19): 10388–10392. doi:10.1073/pnas.93.19.10388. PMC 38394. PMID 8816810.
- ^ Schmitt KC, Reith ME (2011). "The atypical stimulant and nootropic modafinil interacts with the dopamine transporter in a different manner than classical cocaine-like inhibitors". PLOS ONE. 6 (10): e25790. Bibcode:2011PLoSO...625790S. doi:10.1371/journal.pone.0025790. PMC 3197159. PMID 22043293.
- ^ "Sigma Receptors Play Role in Cocaine-induced Suppression of Immune System". Sciencedaily.com. 6 May 2003. Archived from the original on 12 January 2011. Retrieved 9 March 2010.
- ^ Lluch J, Rodríguez-Arias M, Aguilar MA, Miñarro J (November 2005). "Role of dopamine and glutamate receptors in cocaine-induced social effects in isolated and grouped male OF1 mice". Pharmacology Biochemistry and Behavior. 82 (3): 478–87. doi:10.1016/j.pbb.2005.10.003. PMID 16313950. S2CID 13307446.
- ^ Knuepfer MM (March 2003). "Cardiovascular disorders associated with cocaine use: myths and truths". Pharmacology & Therapeutics. 97 (3): 181–222. doi:10.1016/S0163-7258(02)00329-7. PMID 12576134.
- ^ "Drugbank website "drug card", "(DB00907)" for Cocaine: Giving ten targets of the molecule in vivo, including dopamine/serotonin sodium channel affinity & K-opioid affinity". Drugbank.ca. Archived from the original on 20 February 2010. Retrieved 9 March 2010.
- ^ Uz T, Akhisaroglu M, Ahmed R, Manev H (December 2003). "The pineal gland is critical for circadian Period1 expression in the striatum and for circadian cocaine sensitization in mice". Neuropsychopharmacology. 28 (12): 2117–23. doi:10.1038/sj.npp.1300254. PMID 12865893.
- ^ McClung CA, Sidiropoulou K, Vitaterna M, Takahashi JS, White FJ, Cooper DC, et al. (June 2005). "Regulation of dopaminergic transmission and cocaine reward by the Clock gene". Proceedings of the National Academy of Sciences of the United States of America. 102 (26): 9377–81. Bibcode:2005PNAS..102.9377M. doi:10.1073/pnas.0503584102. PMC 1166621. PMID 15967985.
- ^ Aguinaga D, Medrano M, Cordomí A, Jiménez-Rosés M, Angelats E, Casanovas M, et al. (February 2019). "Cocaine Blocks Effects of Hunger Hormone, Ghrelin, Via Interaction with Neuronal Sigma-1 Receptors". Molecular Neurobiology. 56 (2): 1196–1210. doi:10.1007/s12035-018-1140-7. hdl:2445/127306. PMID 29876881. S2CID 46964405.
- ^ Bouhlal S, Ellefsen KN, Sheskier MB, Singley E, Pirard S, Gorelick DA, et al. (November 2017). "Acute effects of intravenous cocaine administration on serum concentrations of ghrelin, amylin, glucagon-like peptide-1, insulin, leptin and peptide YY and relationships with cardiorespiratory and subjective responses". Drug and Alcohol Dependence. 180: 68–75. doi:10.1016/j.drugalcdep.2017.07.033. PMC 5654385. PMID 28881319.
- ^ Carey RJ, Damianopoulos EN, Shanahan AB (January 2008). "Cocaine effects on behavioral responding to a novel object placed in a familiar environment". Pharmacology Biochemistry and Behavior. 88 (3): 265–71. doi:10.1016/j.pbb.2007.08.010. PMID 17897705. S2CID 22711773.
- ^ "Content Background: Chemical Characteristics of Cocaine". duke.edu. Archived from the original on 8 July 2024. Retrieved 4 May 2020.
- ^ a b Humphrey AJ, O'Hagan D (October 2001). "Tropane alkaloid biosynthesis. A century-old problem unresolved". Natural Product Reports. 18 (5): 494–502. doi:10.1039/b001713m. PMID 11699882.
- ^ Amara SB, Koslowski T, Zaidi A (2021). "Quantum Chemistry of Cocaine and its Isomers I: Energetics, Reactivity and Solvation". South African Journal of Chemistry. 75. doi:10.17159/0379-4350/2021/v75a3.
- ^ Drake LR, Scott PJ (October 2018). "DARK Classics in Chemical Neuroscience: Cocaine". ACS Chemical Neuroscience. 9 (10): 2358–2372. doi:10.1021/acschemneuro.8b00117. PMC 6197930. PMID 29630337.
- ^ Dewick PM (2009). Medicinal Natural Products. Chichester: Wiley-Blackwell. ISBN 978-0-470-74276-1.
- ^ Robins RJ, Abraham TE, Parr AJ, Eagles J, Walton NJ (1997). "The Biosynthesis of Tropane Alkaloids in Datura stramonium: The Identity of the Intermediates between N-Methylpyrrolinium Salt and Tropinone". J. Am. Chem. Soc. 119 (45): 10929–10934. Bibcode:1997JAChS.11910929R. doi:10.1021/ja964461p.
- ^ Hoye TR, Bjorklund JA, Koltun DO, Renner MK (January 2000). "N-methylputrescine oxidation during cocaine biosynthesis: study of prochiral methylene hydrogen discrimination using the remote isotope method". Organic Letters. 2 (1): 3–5. doi:10.1021/ol990940s. PMID 10814231.
- ^ Leete E, Bjorklund JA, Couladis MM, Kim SH (1991). "Late intermediates in the biosynthesis of cocaine: 4-(1-methyl-2-pyrrolidinyl)-3-oxobutanoate and methyl ecgonine". J. Am. Chem. Soc. 113 (24): 9286–9292. Bibcode:1991JAChS.113.9286L. doi:10.1021/ja00024a039.
- ^ Leete E, Bjorklund JA, Kim SH (1988). "The biosynthesis of the benzoyl moiety of cocaine". Phytochemistry. 27 (8): 2553–2556. Bibcode:1988PChem..27.2553L. doi:10.1016/0031-9422(88)87026-2.
- ^ Leete E, Marion L, Spenser ID (October 1954). "Biogenesis of hyoscyamine". Nature. 174 (4431): 650–1. Bibcode:1954Natur.174..650L. doi:10.1038/174650a0. PMID 13203600. S2CID 4264282.
- ^ Robins RJ, Waltons NJ, Hamill JD, Parr AJ, Rhodes MJ (October 1991). "Strategies for the genetic manipulation of alkaloid-producing pathways in plants". Planta Medica. 57 (7 Suppl): S27-35. Bibcode:1991PlMed..57S..27R. doi:10.1055/s-2006-960226. PMID 17226220. S2CID 45912704.
- ^ Hemscheidt T, Vederas JC (2000). Leeper FJ, Vederas JC (eds.). "Tropane and Related Alkaloids". Top. Curr. Chem. Topics in Current Chemistry. 209: 175. doi:10.1007/3-540-48146-X. ISBN 978-3-540-66573-1.
- ^ Portsteffen A, Draeger B, Nahrstedt A (1992). "Two tropinone reducing enzymes from Datura stramonium transformed root cultures". Phytochemistry. 31 (4): 1135–1138. Bibcode:1992PChem..31.1135P. doi:10.1016/0031-9422(92)80247-C.
- ^ Boswell HD, Dräger B, McLauchlan WR, Portsteffen A, Robins DJ, Robins RJ, et al. (November 1999). "Specificities of the enzymes of N-alkyltropane biosynthesis in Brugmansia and Datura". Phytochemistry. 52 (5): 871–8. Bibcode:1999PChem..52..871B. doi:10.1016/S0031-9422(99)00293-9. PMID 10626376.
- ^ "Genetically modified tobacco plant produces cocaine in its leaves". New Scientist. Archived from the original on 27 November 2022. Retrieved 27 November 2022.
- ^ "Drug torches 'don't always work'". BBC News. 22 July 2009.
- ^ "Drug torches for bouncers 'don't always spot cocaine'". BBC News. 14 June 2013.
- ^ "Meet the Chemist Behind Many Popular—and Faulty—Police Drug Kits". Pacific Standard. 22 June 2016. Archived from the original on 8 August 2020. Retrieved 21 April 2020.
- ^ Gabrielson R, Sanders T (7 July 2016). "How a $2 Roadside Drug Test Sends Innocent People to Jail". The New York Times. Archived from the original on 1 January 2022. Retrieved 21 April 2020.
- ^ Travnikoff B (1 April 1983). "Semiquantitative screening test for cocaine". Analytical Chemistry. 55 (4): 795–796. doi:10.1021/ac00255a048. ISSN 0003-2700.
- ^ The Cocaine Threat: A Hemispheric Perspective (PDF). United States Department of Defense. Archived from the original (PDF) on 11 September 2008.
- ^ United Nations (June 2010). World Drug Report 2010. United Nations Publications. p. 77. ISBN 978-92-1-148256-0. Archived from the original on 26 April 2016.
- ^ "Annual prevalence of use of drugs, by region and globally, 2016". World Drug Report 2018. United Nations Office on Drugs and Crime. 2018. Retrieved 7 July 2018.
- ^ a b "World Drug Report 2016 (interactive map)". United Nations Office on Drugs and Crime. 2016. Archived from the original on 9 March 2018.
- ^ "Dashboard. Prevalence of cocaine use in Europe (updated June 2024) | www.euda.europa.eu". www.euda.europa.eu.
- ^ a b c d "Cocaine – the current situation in Europe (European Drug Report 2025) | www.euda.europa.eu". www.euda.europa.eu.
- ^ "Cocaine & Crack". Erowid.org. Archived from the original on 6 October 2007. Retrieved 10 July 2007.
- ^ a b "Field Listing – Illicit drugs (by country)". Cia.gov. Archived from the original on 29 December 2010. Retrieved 15 January 2011.
- ^ Franklin J (18 August 2009). "The world's first cocaine bar". The Guardian. ISSN 0261-3077. Archived from the original on 12 January 2017. Retrieved 23 December 2016.
- ^ Grisaffi T. "The Cato Accord: Bolivia's Humane and Effective Approach to Controlling Coca Cultivation" (PDF). ain-bolivia.org. Archived (PDF) from the original on 3 May 2016. Retrieved 12 January 2017.
- ^ "Therapeutic Goods (Poisons Standard—October 2023) Instrument 2023". Federal Register of Legislation. Australian Government. 26 September 2023. Retrieved 22 January 2024.
- ^ "Illicit drug use". Australian Institute of Health and Welfare. 13 December 2023. Archived from the original on 20 January 2024. Retrieved 22 January 2024.
- ^ "Misuse of Drugs Act 1981" (PDF). Western Australian Legislation. Government of Western Australia Department of Justice Parliamentary Counsel's Office. Archived (PDF) from the original on 17 February 2024. Retrieved 22 January 2024.
- ^ a b c d Gootenberg P, ed. (1999). Cocaine: Global Histories. London: Routledge. ISBN 978-0-203-02646-5.
- ^ Madge T (2001). White Mischief: A Cultural History of Cocaine. Edinburgh: Mainstream Publishing Company. p. 106. ISBN 978-1-84018-405-1.
- ^ "Narcotic drug addiction". American Medicine. American-Medicine Publishing Company: 799. November 1915. Archived from the original on 9 May 2018. Retrieved 29 April 2018.
- ^ Brown E, Barganier G (2018). Race and Crime: Geographies of Injustice. Oakland, California: University of California Press. pp. 207–209. ISBN 978-0-520-29418-9. Archived from the original on 12 April 2023. Retrieved 21 November 2021.
- ^ Moore NM (2015). The Political Roots of Racial Tracking in American Criminal Justice. New York, NY: Cambridge University Press. p. 270. ISBN 978-1-107-02297-3. Archived from the original on 6 April 2023. Retrieved 21 November 2021.
- ^ Glaser J (2015). Suspect Race: Causes and Consequences of Racial Profiling. New York, NY: Oxford University Press. p. 7. ISBN 978-0-19-537040-9. Archived from the original on 12 April 2023. Retrieved 21 November 2021.
- ^ May N (22 September 2024). "Should cocaine and MDMA users carry naloxone, the medicine that prevents fatal opioid overdoses?". The Guardian.
- ^ "Treatment of opioid dependence". World Health Organization. WHO. 2014. Archived from the original on 14 March 2014. Retrieved 17 March 2014.
- ^ "Drug use prevention, treatment and care". United Nations Office on Drugs and Crime. UNODC. 2014. Archived from the original on 10 September 2020. Retrieved 17 March 2014.
- ^ Suttles C. "Wyoming's Albertsons, Safeway pharmacies to offer Narcan over the counter". Wyoming Tribune Eagle. Archived from the original on 3 February 2018. Retrieved 19 September 2018.
- ^ Kekatos M (15 May 2024). "Walgreens announces it will sell generic version of over-the-counter Narcan". ABC News. Retrieved 10 August 2024.
- ^ "Is Scott's reagent reliable?". 4 September 2023.
- ^ Bell S (30 June 2004). Dictionary of Forensic Science (Facts on File Science Dictionary) (Facts on File Science Dictionary Series.). Facts on File Inc. p. 142. ISBN 978-0-8160-5131-1. Retrieved 25 January 2012.
- ^ O'Neal CL, Crouch DJ, Fatah AA (1 January 2013). "Validation of Twelve Chemical Spot Tests for the Detection of Drugs of Abuse*". Encyclopedia of Forensic Sciences (Second ed.): 380–387. doi:10.1016/B978-0-12-382165-2.00321-4. ISBN 978-0-12-382166-9. Retrieved 11 January 2022.
- ^ "How to Test Your Drugs With Reagents" (PDF). DanceSafe.
- ^ Webb G (1999). Dark Alliance. Seven Stories Press. p. 35. ISBN 978-1-888363-93-7.
- ^ McSweeney K (June 2020). "Reliable drug war data: The Consolidated Counterdrug Database and cocaine interdiction in the "Transit Zone"". The International Journal on Drug Policy. 80: 102719. doi:10.1016/j.drugpo.2020.102719. PMID 32416537.
- ^ "Cocaine: Seizures, 1998–2003" (PDF). World Drug Report 2006. Vol. 2. New York: United Nations. 2006. Archived (PDF) from the original on 14 June 2007.
- ^ Engelke BF, Gentner WA (January 1991). "Determination of cocaine in "Mate de Coca" herbal tea". Journal of Pharmaceutical Sciences. 80 (1): 96. doi:10.1002/jps.2600800123. PMID 2013859.
- ^ ""Al campesino no le queda otra alternativa que vender su coca al narcotráfico... Enaco paga un bajo precio"". 11 August 2015.
- ^ Busnel R, Manrique López H (July 2023). "The political economy of a failed drug reform: Insights from Peru's main legal coca valley". The International Journal on Drug Policy. 117: 104050. doi:10.1016/j.drugpo.2023.104050. PMID 37267739.
- ^ Benson, Drew. "Coca kick in drinks spurs export fears", The Washington Times, April 20, 2004. Accessed June 14, 2007. "Coke dropped cocaine from its recipe around 1900, but the secret formula still calls for a cocaine-free coca extract produced at a Stepan Co. factory in Maywood, N.J. Stepan buys about 100 metric tons of dried Peruvian coca leaves each year, said Marco Castillo, spokesman for Peru's state-owned National Coca Co."
- ^ May, Clifford D. "How Coca-Cola Obtains Its Coca", The New York Times, July 1, 1988. Accessed April 11, 2008. "A Stepan laboratory in Maywood, N.J., is the nation's only legal commercial importer of coca leaves, which it obtains mainly from Peru and, to a lesser extent, Bolivia. Besides producing the coca flavoring agent sold to The Coca-Cola Company, Stepan extracts cocaine from the coca leaves, which it sells to Mallinckrodt Inc., a St. Louis pharmaceutical manufacturer that is the only company in the United States licensed to purify the product for medicinal use." See links for more information
- ^ "Mallinckrodt Pharmaceuticals – Compounding Powders – Cocaine Hydrochloride USP CII". Mallinckrodt Pharmaceuticals.
- ^ a b "Coke light: drug tests show 40% of 'cocaine' had no cocaine | Australian National University". www.anu.edu.au. 25 August 2022.
- ^ "Colombia". CIA World Factbook. Archived from the original on 18 June 2021. Retrieved 24 January 2021.
- ^ "Peru Overtakes Colombia as Top Cocaine Producer". NBC News. 31 July 2012. Archived from the original on 4 March 2016.
- ^ Ciro E, Ryder M, Sánchez S (2024). "Peace and reparations in legal drug markets in Colombia". Futures. 157: 103336. doi:10.1016/j.futures.2024.103336.
- ^ "National Drug Threat Assessment 2006". National Drug Intelligence Center. 2006. Archived from the original on 11 November 2010.
- ^ "Cocaine Seized Worldwide Highest Ever in 2011". Flare Network (Flarenetwork.org). 18 January 2012. Archived from the original on 6 January 2014. Retrieved 5 January 2014.
- ^ "Colombia". U.S. Department of State. State.gov. Archived from the original on 22 January 2017. Retrieved 26 March 2013.
- ^ a b c d e f g h i j k l m n o p q r Drug Enforcement Administration Office of Intelligence Strategic Intelligence Section Latin America Unit (1991). Coca Cultivation and Cocaine Processing:An Overview (PDF) (Report). Washington, D.C.: U.S. Department of Justice, Drug Enforcement Administration.
- ^ Messina JP, Delamater PL (10 January 2006). "Defoliation and the war on drugs in Putumayo, Colombia". International Journal of Remote Sensing. 27 (1): 121–128. Bibcode:2006IJRS...27..121M. doi:10.1080/01431160500293708. ISSN 0143-1161.
- ^ Ferreira JF, Smeda RJ, Duke SO (1997). "Control of coca plants ( Erythroxylum coca and E. novogranatense ) with glyphosate". Weed Science. 45 (4): 551–556. Bibcode:1997WeedS..45..551F. doi:10.1017/S0043174500088809. ISSN 0043-1745.
- ^ Marcela I (August 2010). "Who crops coca and why? The case of Colombian farmers" (PDF). Econstor. Archived (PDF) from the original on 28 April 2024. Retrieved 28 April 2024.
- ^ "Colombia: 'I'm not proud cultivating coca, but we have no choice'". Al Jazeera. Archived from the original on 8 July 2024. Retrieved 28 April 2024.
- ^ Siegel RK (1985). "New Patterns of Cocaine Use: Changing Doses and Routes". In Kozel NJ, Adams EH (eds.). Cocaine Use in America: Epidemiologic and Clinical Perspectives (PDF). NIDA Research Monograph. Vol. 61. U.S. Dept. of Health and Human Services. pp. 204–222. Archived from the original (PDF) on 9 October 2016. Retrieved 9 April 2016.
- ^ A. Arif, ed. (1987), Adverse health consequences of cocaine abuse (PDF), World Health Organization
- ^ Streatfeild D (2003). Cocaine: An Unauthorized Biography. Macmillan. ISBN 978-0-312-42226-4. Archived from the original on 15 January 2014. Retrieved 5 January 2014.
- ^ "How Much Is a Gram of Coke?". New Health Advisor. 3 September 2015. Archived from the original on 7 March 2017.
- ^ a b Woody C (5 April 2017). "Fake vegetables, bananas, drones and pastries – here are some of drug smuggler's most bizarre methods". Business Insider. Retrieved 22 May 2020.
- ^ "Poland seizes liquid cocaine worth $1.9 MLN in wine shipment". Reuters. 17 December 2024.
- ^ McNicholas MA (2016). Maritime Security, 2nd Edition. Butterworth-Heinemann. p. 222.
- ^ "Writhing shipment yeilds smuggled cocaine - UPI Archives". UPI.
- ^ Esposito R (2 February 2009). "Exotic animals trapped in net of drug trade". Reuters. Retrieved 10 June 2025.
- ^ a b Pressly L (24 November 2015). "The Mochileros". BBC News. Retrieved 24 November 2015.
- ^ "Cruzan desierto con pacas de droga en la espalda".
- ^ a b Fleetwood J (18 June 2014). Drug Mules. Springer. ISBN 978-1-137-27190-7.
- ^ "Drug mules: Swallowed by the illicit drug trade". UN Office of Drugs and Crime. Archived from the original on 8 July 2024. Retrieved 29 June 2024.
- ^ "75-year-old man arrested after $930K in cocaine found hidden in vehicle seats". CBS Austin. 13 May 2025.
- ^ Zamora K (16 May 2025). "Court documents: Nearly $500K worth of cocaine found at Amarillo bus station". newschannel10.
- ^ "Man caught smuggling cocaine in his clothes at Brussels Airport". The Brussels Times.
- ^ Abuja NK (22 December 2024). "NDLEA arrests businessman at Kano airport for body packing large consignment of cocaine". The Nation Newspaper.
- ^ "Drug smuggler who swallowed kilo of cocaine worth Dh5 million arrested at Abu Dhabi airport". The National.
- ^ Resiere D, Mehdaoui H, Megarbane B (6 January 2019). "Cardiac Arrest in the Airport Revealing Cocaine Body Packing: A Case Report". Case Reports in Medicine. 2019: 6183154. doi:10.1155/2019/6183154. PMC 6339722. PMID 30723506.
- ^ Klein A, Day M, Harriott A (18 July 2013). Caribbean Drugs. Zed Books Ltd. ISBN 978-1-84813-622-9.
- ^ Sutton H (August 2020). "3 Types Of Go-Fast Narco Boats The Coast Guard Faces". Forbes. Archived from the original on 6 February 2024. Retrieved 29 June 2024.
- ^ "Coast Guard hunts drug-running semi-subs". CNN. 20 March 2008. Archived from the original on 21 March 2008. Retrieved 20 March 2008.
- ^ "Drug smuggling: Underwater drones seized by Spanish police". 4 July 2022.
- ^ "Spanish police confiscate three underwater drones designed to transport large quantities of drugs". Telegrafi (via Reuters). Madrid. Reuters. 5 July 2022. Retrieved 17 June 2025.
- ^ Agence France-Presse-AFP (5 July 2022). "Spanish police bust first underwater drug smuggling drones". Daily Sabah.
- ^ "Drug cartels use mini whale submarines to smuggle cocaine into Australia via Cyprus". The Greek Herald. 6 January 2025.
- ^ a b Daly M (30 April 2025). "Cocaine, corruption and bribes: the German port under siege by Europe's criminal drug gangs". The Guardian.
- ^ a b "Cocaine, corruption and bribery, the German port surrounded by drug gangs". KOHA.net. 6 May 2025.
- ^ "Cocaine. Puerto Rico and the U.S. Virgin Islands Drug Threat Assessment". National Drug Intelligence Center. 2003. Archived from the original on 29 June 2024. Retrieved 29 June 2024.
- ^ Zimmerman S (23 October 2012). A History of Smuggling in Florida. Arcadia Publishing. ISBN 978-1-61423-356-5.
- ^ Corben B, Spellman A (May 2009). Cocaine Cowboys. powerHouse Books. ISBN 978-1-57687-503-2.
- ^ "The Cocaine Pipeline to Europe" (PDF). Global Initiative. February 2021. Retrieved 29 June 2024.
- ^ United Nations Office on Drugs and Crime (16 December 2015). World Drug Report 2015. United Nations. p. XV. ISBN 978-92-1-057300-9.
- ^ Jacobson R (2006). Illegal drugs: America's anguish (2005 ed.). Farmington Hills, Michigan: Thomson Gale. p. 82. ISBN 978-1-4144-0419-6.
- ^ "2015 National Drug Threat Assessment Summary" (PDF). Drug Enforcement Administration. United States Department of Justice: Drug Enforcement Administration. October 2015. pp. 1–2. Archived from the original (PDF) on 10 April 2016. Retrieved 10 April 2016.
Mexican TCOs pose the greatest criminal drug threat to the United States; no other group is currently positioned to challenge them. These Mexican poly-drug organizations traffic heroin, methamphetamine, cocaine, and marijuana throughout the United States, using established transportation routes and distribution networks. ... While all of these Mexican TCOs transport wholesale quantities of illicit drugs into the United States, the Sinaloa Cartel appears to be the most active supplier. The Sinaloa Cartel leverages its expansive resources and dominance in Mexico to facilitate the smuggling and transportation of drugs throughout the United States.
- ^ "Meth Info". Methproject.org. Archived from the original on 27 March 2010.
- ^ "Drugs of Abuse". City of Denison Iowa. Archived from the original on 6 November 2011. Retrieved 13 November 2011.
- ^ "Cocaine prices" (PDF). Office on Drugs and Crime. United Nations.
- ^ "Drugs: Pricing Power". The Economist. 28 June 2007. Archived from the original on 6 January 2014.
Prices: USA around $110/g, Israel/Germany/Britain around $46/g, Colombia $2/g, New Zealand recordbreaking $714.30/g.
- ^ European Monitoring Centre for Drugs and Drug Addiction (2008). Annual report: the state of the drugs problem in Europe (PDF). Luxembourg: Office for Official Publications of the European Communities. p. 59. ISBN 978-92-9168-324-6. Archived (PDF) from the original on 25 April 2013. Retrieved 31 December 2013.
- ^ "Sniffing out a fruit-flavored trend in cocaine". NBC News. 17 April 2008.
- ^ a b Wagner KD, Fiuty P, Page K, Tracy EC, Nocera M, Miller CW, et al. (November 2023). "Prevalence of fentanyl in methamphetamine and cocaine samples collected by community-based drug checking services". Drug and Alcohol Dependence. 252: 110985. doi:10.1016/j.drugalcdep.2023.110985. PMC 10688611. PMID 37826988.
- ^ Pillay VV (2013), Modern Medical Toxicology (4th ed.), Jaypee, pp. 553–554, ISBN 978-93-5025-965-8
- ^ Prieto JP, Scorza C, Serra GP, Perra V, Galvalisi M, Abin-Carriquiry JA, et al. (August 2016). "Caffeine, a common active adulterant of cocaine, enhances the reinforcing effect of cocaine and its motivational value". Psychopharmacology. 233 (15–16): 2879–2889. doi:10.1007/s00213-016-4320-z. hdl:20.500.12381/203. PMID 27270948.
- ^ "Statistical Bulletin 2024 — price, purity and potency | www.euda.europa.eu". European Union Drugs Agency. Retrieved 25 February 2025.
- ^ Ribeiro M, Trevizol AP, Frajzinger R, Ribeiro A, Speierl H, Pires L, et al. (July 2019). "Adulterants in crack cocaine in Brazil". Trends in Psychiatry and Psychotherapy. 41 (2): 186–190. doi:10.1590/2237-6089-2017-0143. PMID 31314858.
- ^ United Nations Office on Drugs and Crime. Laboratory and Scientific Section (2005). Methods for Impurity Profiling of Heroin and Cocaine. United Nations Publications. ISBN 978-92-1-148206-5.
- ^ EMCDDA (2007). "EMCDDA Retail Cocaine Purity Study". Archived from the original on 1 January 2014. Retrieved 31 December 2013.
- ^ Centers for Disease Control Prevention (CDC) (December 2009). "Agranulocytosis associated with cocaine use - four States, March 2008-November 2009". MMWR. Morbidity and Mortality Weekly Report. 58 (49): 1381–5. PMID 20019655.
- ^ Moisse K (23 June 2011). "Cocaine Laced With Veterinary Drug Levamisole Eats Away at Flesh". ABC News. Archived from the original on 25 June 2011. Retrieved 23 June 2011.
- ^ Solomon N, Hayes J (September 2017). "Levamisole: A High Performance Cutting Agent". Academic Forensic Pathology. 7 (3): 469–476. doi:10.23907/2017.039. PMC 6474566. PMID 31239995.
- ^ Rothman RB, Baumann MH (July 2002). "Therapeutic and adverse actions of serotonin transporter substrates". Pharmacol Ther. 95 (1): 73–88. doi:10.1016/s0163-7258(02)00234-6. PMID 12163129.
- ^ Rothman RB, Baumann MH (2006). "Therapeutic potential of monoamine transporter substrates". Curr Top Med Chem. 6 (17): 1845–1859. doi:10.2174/156802606778249766. PMID 17017961.
- ^ Rothman RB, Baumann MH (April 2002). "Serotonin releasing agents. Neurochemical, therapeutic and adverse effects". Pharmacol Biochem Behav. 71 (4): 825–836. doi:10.1016/s0091-3057(01)00669-4. PMID 11888573.
- ^ Bernardo NP, Siqueira ME, De Paiva MJ, Maia PP (2003). "Caffeine and other adulterants in seizures of street cocaine in Brazil". International Journal of Drug Policy. 14 (4): 331–4. doi:10.1016/S0955-3959(03)00083-5.
- ^ "UNITED STATES of America, Plaintiff-Appellee, v. Luis A. CUELLO, Alvaro Bastides-Benitez, John Doe, a/k/a Hugo Hurtado, and Alvaro Carvajal, Defendants-Appellants". Docket No. 78-5314. United States Court of Appeals, Fifth Circuit. 25 July 1979. Archived from the original on 24 May 2012.
- ^ "Procaine". ecstasydata.org.
- ^ "Cocaína 'envenenada' que causou mortes na Argentina tinha anestésico para elefantes". G1 (in Brazilian Portuguese).
- ^ Barratt M, Lee N (15 July 2024). "Cocaine is being contaminated with powerful opioids called nitazenes. Here's why it's a dangerous mix". The Conversation.
- ^ Rachwani M (25 August 2022). "Australia's first government-backed pill testing clinic finds 40% of 'cocaine' contained no coke". The Guardian.
- ^ "How the drug wars impact Latin America and the Caribbean development? | Feature from King's College London". www.kcl.ac.uk.
- ^ Janda KD, Treweek JB (December 2011). "Vaccines targeting drugs of abuse: is the glass half-empty or half-full?". Nature Reviews. Immunology. 12 (1): 67–72. doi:10.1038/nri3130. PMID 22173478.
- ^ Anthenelli RM, Somoza E (September 2010). "Vaccine for cocaine addiction: A promising new immunotherapy" (PDF). Current Psychiatry. 9 (9): 16–20.
- ^ Bremer PT, Schlosburg JE, Banks ML, Steele FF, Zhou B, Poklis JL, et al. (June 2017). "Development of a Clinically Viable Heroin Vaccine". Journal of the American Chemical Society. 139 (25): 8601–8611. Bibcode:2017JAChS.139.8601B. doi:10.1021/jacs.7b03334. PMC 5612493. PMID 28574716.
- ^ Teobaldo L (1994). "The Standard Low Dose of Oral Cocaine: Used for Treatment of Cocaine Dependence" (PDF). Substance Abuse. 15 (4): 215–220. Archived (PDF) from the original on 2 June 2014.
- ^ Mariani JJ, Khantzian EJ, Levin FR (March 2014). "The self-medication hypothesis and psychostimulant treatment of cocaine dependence: an update". The American Journal on Addictions. 23 (2): 189–193. doi:10.1111/j.1521-0391.2013.12086.x. PMC 4227391. PMID 25187055.
- ^ Kandel ER, Kandel DB (September 2014). "Shattuck Lecture. A molecular basis for nicotine as a gateway drug". The New England Journal of Medicine. 371 (10): 932–943. doi:10.1056/NEJMsa1405092. PMC 4353486. PMID 25184865.
- ^ Keyes KM, Hamilton A, Kandel DB (June 2016). "Birth Cohorts Analysis of Adolescent Cigarette Smoking and Subsequent Marijuana and Cocaine Use". American Journal of Public Health. 106 (6): 1143–1149. doi:10.2105/AJPH.2016.303128. PMC 4880234. PMID 27077359.
- ^ Ren M, Lotfipour S (August 2019). "Nicotine Gateway Effects on Adolescent Substance Use". The Western Journal of Emergency Medicine. 20 (5): 696–709. doi:10.5811/westjem.2019.7.41661. PMC 6754186. PMID 31539325.
- ^ Griffin EA, Melas PA, Zhou R, Li Y, Mercado P, Kempadoo KA, et al. (November 2017). "Prior alcohol use enhances vulnerability to compulsive cocaine self-administration by promoting degradation of HDAC4 and HDAC5". Science Advances. 3 (11): e1701682. Bibcode:2017SciA....3E1682G. doi:10.1126/sciadv.1701682. PMC 5665598. PMID 29109977.
- ^ Anderson EM, Penrod RD, Barry SM, Hughes BW, Taniguchi M, Cowan CW (August 2019). "It is a complex issue: emerging connections between epigenetic regulators in drug addiction". The European Journal of Neuroscience. 50 (3): 2477–2491. doi:10.1111/ejn.14170. PMID 30251397. S2CID 52816486.
- ^ Lopez-Quintero C, Pérez de los Cobos J, Hasin DS, Okuda M, Wang S, Grant BF, et al. (May 2011). "Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC)". Drug and Alcohol Dependence. 115 (1–2): 120–130. doi:10.1016/j.drugalcdep.2010.11.004. PMC 3069146. PMID 21145178.
- ^ Bickel WK, Snider SE, Quisenberry AJ, Stein JS, Hanlon CA (2016). "Competing neurobehavioral decision systems theory of cocaine addiction". Competing neurobehavioral decision systems theory of cocaine addiction: From mechanisms to therapeutic opportunities. Progress in Brain Research. Vol. 223. pp. 269–293. doi:10.1016/bs.pbr.2015.07.009. ISBN 978-0-444-63545-7. PMC 5495192. PMID 26806781.
- ^ Dimitrijevic N, Dzitoyeva S, Manev H (August 2004). "An automated assay of the behavioral effects of cocaine injections in adult Drosophila". Journal of Neuroscience Methods. 137 (2): 181–184. doi:10.1016/j.jneumeth.2004.02.023. PMID 15262059. S2CID 19882594.
- ^ Martell BA, Mitchell E, Poling J, Gonsai K, Kosten TR (July 2005). "Vaccine pharmacotherapy for the treatment of cocaine dependence". Biol. Psychiatry. 58 (2): 158–64. doi:10.1016/j.biopsych.2005.04.032. PMID 16038686. S2CID 22415520.
- ^ Hesse M (2002). Alkaloids: Nature's Curse or Blessing?. Weinheim: Wiley-VCH. p. 304. ISBN 978-3-906390-24-6.
- ^ Dillehay TD, Rossen J, Ugent D, Karathanasis A, Vásquez V, Netherly PJ (2010). "Early Holocene coca chewing in northern Peru". Antiquity. 84 (326): 939–953. doi:10.1017/S0003598X00067004. ISSN 0003-598X.
- ^ Altman AJ, Albert DM, Fournier GA (1985). "Cocaine's use in ophthalmology: our 100-year heritage". Survey of Ophthalmology. 29 (4): 300–6. doi:10.1016/0039-6257(85)90153-5. PMID 3885453.
- ^ Gay GR, Inaba DS, Sheppard CW, Newmeyer JA (1975). "Cocaine: history, epidemiology, human pharmacology, and treatment. a perspective on a new debut for an old girl". Clinical Toxicology. 8 (2): 149–78. doi:10.3109/15563657508988061. PMID 1097168.
- ^ "Drug that spans the ages: The history of cocaine". London: The Independent (UK). 2006. Archived from the original on 28 February 2010. Retrieved 30 April 2010.
- ^ Monardes N, Frampton J (1925). Joyfull Newes out of the Newe Founde Worlde. New York: Alfred Knopf.
- ^ "InterAndean Institute of Coca Sciences". www.cienciadelacoca.org. Archived from the original on 30 December 2016.
- ^ Karch SB (May 1998). A Brief History of Cocaine. Boca Raton, Fla: CRC Press. ISBN 978-0-8493-4019-2.
- ^ Luch A (3 April 2009). Molecular, Clinical and Environmental Toxicology. Basel Boston: Springer Science & Business Media. p. 20. ISBN 978-3-7643-8336-7.
- ^ Gaedcke F (1855). "Ueber das Erythroxylin, dargestellt aus den Blättern des in Südamerika cultivirten Strauches Erythroxylon Coca". Archiv der Pharmazie. 132 (2): 141–150. doi:10.1002/ardp.18551320208. S2CID 86030231. Archived from the original on 14 April 2021. Retrieved 3 September 2020.
- ^ a b Niemann A (1860). "Ueber eine neue organische Base in den Cocablättern". Archiv der Pharmazie. 153 (2 and 3): 129–155, 291–308. doi:10.1002/ardp.18601530202. S2CID 98195820. Archived from the original on 28 July 2020. Retrieved 30 June 2019.
- ^ Harper D. "Cocaine". Online Etymology Dictionary.
- ^ Singh S (March 2000). "Chemistry, design, and structure-activity relationship of cocaine antagonists" (PDF). Chemical Reviews. 100 (3): 925–1024. doi:10.1021/cr9700538. PMID 11749256. Archived (PDF) from the original on 4 March 2016.
Page 970 (46th page of article) first, ninth, and tenth lines
- ^ (a) Willstatter R (1903). "Synthese der Ecgoninsäure" [Synthesis of Tropine]. Liebigs Ann. (in German). 326 (1–2): 23. doi:10.1002/jlac.19033260105. (b) Robinson RJ (1917). "LXIII. A synthesis of tropinone". J. Chem. Soc., Trans. 111: 762–768. doi:10.1039/CT9171100762. Archived from the original on 30 September 2020. Retrieved 30 June 2019. (c) Schopf C, Lehman G (1935). "Die Synthese des Tropinons, Pseudopelletierins, Lobelanins und verwandter Alkaloide unter physiologischen Bedingungen" [The synthesis of tropinone, pseudopelletierin, lobelanin and related alkaloids under physiological conditions]. Liebigs Ann. (in German). 518: 1–37. doi:10.1002/jlac.19355180102.
- ^ Yentis SM, Vlassakov KV (March 1999). "Vassily von Anrep, forgotten pioneer of regional anesthesia". Anesthesiology. 90 (3): 890–5. doi:10.1097/00000542-199903000-00033. PMID 10078692.
- ^ Halsted W (1885). "Practical comments on the use and abuse of cocaine". New York Medical Journal. 42: 294–295.
- ^ Corning JL (1885). "An experimental study". New York Medical Journal. 42: 483.
- ^ "Experience Vin Mariani today | Grupo Mariani S.A". Cocanaturally.com. Archived from the original on 8 February 2011. Retrieved 15 January 2011.
- ^ Freud S (1975). Byck R (ed.). Cocaine Papers. Stonehill. ISBN 0-88373-010-3.
- ^ "How a Young Sigmund Freud Researched & Got Addicted to Cocaine, the New "Miracle Drug," in 1894". Open Culture. Archived from the original on 7 March 2017.
- ^ "Sigmund Freud and Cocaine". cocaine.org. Archived from the original on 19 January 2017.
- ^ Musto DF (1989). "America's First Cocaine Epidemic". The Wilson Quarterly. 13 (3): 59–64. JSTOR 40257908. PMID 11619697. Archived from the original on 12 July 2022. Retrieved 12 July 2022.
- ^ "Coca-Cola's cocaine connection is worth billions". National Post. 12 April 2023.
- ^ Barlow W (1989). Looking Up At Down: The Emergence of Blues Culture. Philadelphia: Temple University Press. p. 207. ISBN 0-87722-583-4.
- ^ Streatfeild D (2003). Cocaine: An Unauthorized Biography. Picador. ISBN 978-0-312-42226-4.
- ^ White T (14 August 1993). "Catchin' Cab: The Magic of Calloway". Billboard. p. 3. Archived from the original on 8 July 2024. Retrieved 13 January 2022.
- ^ The Big Broadcast (1932) (Full Movie). 8 January 2021. Event occurs at 1:20:29. Archived from the original on 13 January 2022. Retrieved 13 January 2022 – via YouTube.
- ^ "Jeevan Vasagar: cocaine-based "wonder drug" tested on concentration camp inmates". Amphetamines.com. 19 November 2002. Archived from the original on 27 February 2011. Retrieved 15 January 2011.
- ^ "The Cocaine Energy Drink". www.drinkcocaine.com. 3 October 2006. Archived from the original on 4 October 2006. Retrieved 5 July 2019.
- ^ Chan S (3 October 2006). "Lawmakers Scold Maker of 'Cocaine' Drink". The New York Times. ISSN 0362-4331. Retrieved 5 July 2019.
- ^ Campbell CA (22 September 2006). "Latest energy drink gets some bad buzz". The Seattle Times. Retrieved 5 July 2019.
- ^ "Evo Morales launches 'Coca Colla'". London: Telegraph. 10 January 2010. Retrieved 22 January 2010.
- ^ "Bolivia banks on 'Coca Colla,' fizzy coca-leaf drink". AFP. 10 January 2010. Archived from the original on 15 January 2010. Retrieved 22 January 2010.
- ^ a b Ryzik M (10 June 2007). "Cocaine: Hidden in Plain Sight". The New York Times. Archived from the original on 11 August 2017. Retrieved 18 May 2017.
- ^ "The Buyers – A Social History of America's Most Popular Drugs". FRONTLINE. PBS. Archived from the original on 14 May 2017. Retrieved 18 May 2017.
- ^ Brisbane FL, Womble M (1985). Treatment of Black Alcoholics. Psychology Press. ISBN 978-0-86656-403-8. Archived from the original on 10 September 2017. Retrieved 18 May 2017.
- ^ Waldorf D, Reinarman C, Murphy S (June 1992). Cocaine Changes: The Experience of Using and Quitting. Temple University Press. p. 95. ISBN 978-1-56639-013-2. Retrieved 18 May 2017.
- ^ a b Current JD. "Cocaine". Pharmacology for Anesthetists. p. 27.
- ^ Kozel NJ, Adams EH (July 1996). Cocaine Use in America. DIANE Publishing. ISBN 978-0-7881-2968-1.
- ^ Spillane JF (11 January 2000). Cocaine. Baltimore, MD: JHU Press. ISBN 978-0-8018-6230-4.
- ^ Kilmer B (2017). "Mixed messages: Is cocaine consumption in the U.S. going up or down?". Brookings. Archived from the original on 29 June 2024. Retrieved 29 June 2024.
- ^ Great Britain: Parliament: House of Commons: Home Affairs Committee (3 March 2010). The cocaine trade. The Stationery Office. p. 22. ISBN 978-0-215-54425-4.
- ^ "Apple Sanity – Fetish – Blow: War on Drugs VS. Cocaine". Applesanity.com. 17 June 2008. Archived from the original on 17 June 2008. Retrieved 13 November 2011.
- ^ "Cocaine Market". Havocscope.com. 28 April 2008. Archived from the original on 11 November 2012. Retrieved 9 March 2010.
- ^ WHO/UNICRI (4 February 2010). "The WHO Cocaine Project". Transnational Institute. Archived from the original on 9 August 2012. Retrieved 8 June 2012.
- ^ "Cocaine use doubles in a decade". Sydney Morning Herald. 15 October 2010. Archived from the original on 18 October 2010. Retrieved 19 October 2010.
- ^ "Cocaine". American Heritage Dictionary. Archived from the original on 3 January 2023. Retrieved 3 January 2023.
Further reading
[edit]- Spillane JF, ed. (2000). Cocaine: From Medical Marvel to Modern Menace in the United States, 1884–1920. Baltimore and London: The Johns Hopkins University Press. ISBN 978-0-8018-6230-4.
- Feiling T (2009). The Candy Machine: How Cocaine Took Over the World. London: Penguin. ISBN 978-0-14-103446-1.
External links
[edit]
Cocaine at Wikipedia's sister projects
 Definitions from Wiktionary
Definitions from Wiktionary Media from Commons
Media from Commons Quotations from Wikiquote
Quotations from Wikiquote Data from Wikidata
Data from Wikidata
- Virginia Gewin: Smoking stokes cocaine cravings: Molecular mechanism found for controversial 'gateway drug' hypothesis, Nature News, November 2, 2011.
Licensed under CC BY-SA 3.0 | Source: https://en.wikipedia.org/wiki/Cocaine56 views | Status: cached on June 21 2025 05:49:09↧ Download as ZWI file
 EncycloReader
is supported by the
EncycloReader
is supported by the