Drowning And Life Saving
") From Britannica 11th Edition (1911)
From Britannica 11th Edition (1911) Drowning And Life Saving. To “drown” (a verb used both transitively and intransitively, of which the origin, though traced to earlier forms, is unknown) is to suffer or inflict death by submersion in water, or figuratively to submerge entirely in water or some other liquid. As a form of ancient capital punishment, the method of drowning is referred to at the end of this article, but the interest of the subject is mainly associated with rescue-work in cases of accident.
Death from drowning is the result of asphyxia, due to the stoppage of a supply of fresh air to the lungs. There is a certain amount of stationary air in the lungs, and into this is diffused oxygen from the fresh air taken in, while the carbonic acid which it has taken from the blood through the walls of the capillaries is driven out. This process of exchange is ever proceeding, the whole of it being regulated from the nervous centre at the base of the brain. When a person gets under water and cannot swim, there is a natural tendency to struggle, and in the efforts to respire water is drawn into the windpipe and cough is brought on. This expels the air from the lungs with the water which threatened to suffocate him, and as further efforts are made to respire more water is taken in and has to be swallowed. Meanwhile, the oxygen in the lungs is gradually diminishing, the quantity of carbonic acid is increasing, and at length the air in the lungs becomes too impure to effect an exchange with the blood. Then the blood passing into the heart becomes venous and the heart begins to send out venous instead of arterial blood to all parts of the body. Immediately a dull, sickening pain becomes apparent at the base of the neck, and insensibility rapidly ensues. This arises from the affection of the respiratory nerve centre. In a short space of time the face becomes dark and congested through the veins being gorged with blood, and the heart ultimately ceases to beat.
 |
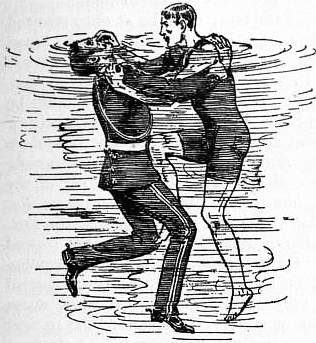
| Fig. 1.—1st Release Method. |
When a person unable to swim falls into the water, he usually rises to the surface, throws up his arms and calls for help. This, with the water swallowed, will make him sink, and if the arms are moved above the head when under water, he will, as a natural consequence, sink still lower. The struggle will be prolonged a few seconds, and then probably cease for a time, allowing him to rise again, though perhaps not sufficiently high to enable him to get another breath of air. If still conscious, he will renew his struggle, more feebly perhaps, but with the same result. As soon as insensibility occurs, the body sinks altogether, owing to the loss of air and the filling of the stomach with water. There is a general belief that a drowning person must rise three times before he finally sinks, but this is a fallacy. The question whether he rises at all, or how often he does so, entirely depends upon circumstances. A man may get entangled among weeds, which prevent his coming to the surface, or he may die through heart failure from the shock or fright of entering the water.
On seeing a person struggling in the water in danger of drowning, no time should be lost in going to his assistance, for he may sink at once, and then there is danger of missing the body when searching under water for it, or it may get entangled among weeds and then the rescuer’s task is rendered doubly dangerous. Before diving in to the rescue the boots and heavy clothing should be discarded if possible, and in cases where a leap has to be made from a height, such as a bridge, high embankment, vessel or pier, or where the depth of the water is not known, it is best to drop in feet first. Where weeds abound there is always danger of entanglement, and therefore progress should be made in the direction of the stream. When approaching a drowning man there is always the danger of being clutched, but a swimmer who knows the right way to deal with a man in the water can easily avoid this; but if through some mistake he finds himself seized by the drowning person, a necessary thing for the swimmer to do is to take advantage of his knowledge of the water and keep uppermost, as this weakens the drowning person and makes the effort of effecting a release much easier than would otherwise be the case. To the Royal Life Saving Society in England is due the credit of disseminating, throughout the entire world, the ideas of swimmers, based on practical experience, as to the safest methods which should be adopted for release and rescue, and their methods, as well as the approved ones for resuscitation, are now taught in almost every school and college.
 |
| Fig. 2.—2nd Release Method. |
 |
| Fig. 3.—3rd Release Method. |
 |
| Fig. 4.—Easiest method of carrying a person not struggling. |
If the rescuer be held by the wrists, he must turn both arms simultaneously against the drowning person’s thumbs, and bring his arms at right angles to the body, thus dislocating the thumbs of the drowning person if he does not leave go (fig. 1). If he be clutched round the neck he must take a deep breath and lean well over the drowning person, at the same time placing one hand in the small of his back, then raise the other arm in line with the shoulder, and pass it over the drowning person’s arm, then pinch the nostrils close with the fingers, and at the same time place the palm of the hand on the chin and push away with all possible force. By the firm holding of the nose the drowning person is made to open his mouth for breathing, and as he will then be under water, choking ensues and he gives way to the rescuer, who then gains complete control (fig. 2). One of the most dangerous clutches is that round the body and arms or round the body only. When so tackled the rescuer should lean well over the drowning person, take a breath as before, and either withdraw both arms in an upward direction in front of his body, or else act in the same way as when releasing oneself when clutched round the neck. In any case one hand must be placed on the drowning man’s shoulder, and the palm of the other hand against his chin, and at the same time one knee should be brought up against the lower part of his chest. Then, with a strong and sudden push, the arms and legs should be stretched out straight and the whole weight of the body thrown backwards. This sudden and totally unexpected action will break the clutch and leave the rescuer free to get hold of the drowning person in such a manner as to be able to bring him to land (fig. 3).
There are several practical methods of carrying a person through the water, the easiest assistance to render being that to a swimmer attacked by cramp or exhaustion, or a drowning person who may be obedient and remain quiet when approached and assured of safety. Then the person assisted should place his arms on the rescuer’s shoulders, close to the neck, with the arms at full stretch, lie on his back perfectly still, with the head well back. The rescuer will then be uppermost, and having his arms and legs free can, with the breast stroke, make rapid progress to the shore; indeed a good pace can easily be made (fig. 4). In
this, as in the other methods afterwards described, every care should be taken to keep the face of the drowning person above the water. All jerking, struggling or tugging should be avoided, and the stroke of the legs be regular and well timed, thus husbanding strength for further effort. The drowning person being able to breathe with freedom is reassured, and is likely to cease struggling, feeling that he is in safe hands.
 |
| Fig. 5.—1st Rescue Method. |
When a drowning person is not struggling, but yet seems likely to do so when approached, the best method of rescue is to swim straight up, turn him on his back, and then place the hands on either side of his face. Then the rescuer should lie on his back, holding the drowning man in front of him, and swim with the back stroke, always taking care to keep the man’s face above water (fig. 5). If the man be struggling and in a condition difficult to manage, he should be turned on his back as before, and a firm hold taken of his arms just above his elbows. Then the man’s arms should be drawn up at right angles to his body and the rescuer should start swimming with the back stroke (fig. 6). He should take particular care not to go against the current or stream, and thereby avoid exhaustion. If the arms be difficult to grasp, or the struggling so violent as to prevent a firm hold, the rescuer should slip his hands under the armpits of the drowning person, and place them on his chest or round his arms, then raise them at right angles to his body, thus placing the drowning person completely in his power. The journey to land can then be made by swimming on the back as in the other methods (fig. 7). In carrying a person through the water, it will be of much advantage to keep his elbows well out from the sides, as this expands the chest, inflates the lungs and adds to his buoyancy. The legs should be kept well up to the surface and the whole body as horizontal as possible. This avoids a drag through the water, and will considerably help the rescuer. In some cases it may happen that the drowning person has sunk to the bottom and does not rise again. In that event the rescuer should look for bubbles rising to the surface before diving in. In still water the bubbles rise perpendicularly; in running water they rise obliquely, so that the rescuer must look for his object higher up the stream than where the bubbles rise. It is also well to remember that in running water a body may be carried along by the current and must be looked for in the direction in which it flows. When a drowning person is recovered on the bottom, the rescuer should seize him by the head or shoulders, place the left foot on the ground and the right knee in the small of his back, and then, with a vigorous push, come to the surface.
 |
| Fig. 6.—2nd Rescue Method. |
 |
| Fig. 7.—3rd Rescue Method. |
When the rescuer reaches land with an insensible person, no time should be lost in sending for a medical man, but in the meantime an attempt to induce artificial respiration may be made. The first recorded cases of resuscitating the apparently drowned are mentioned in the notes to William Derham’s Physico-Theology, as having occurred at Troningholm and Oxford, about 1650. In 1745 Dr J. Fothergill read a paper on the subject before the Royal Society. It dealt with the recovery of a man dead in appearance by distending the lungs by Mr William Tossack, surgeon in Alloa, in 1744. In 1767 several cases of resuscitation were reported in Switzerland, and shortly after a society was formed at Amsterdam for recovery of the apparently drowned, and to instruct the common people as to the best manner of treating them when rescued, and to reward the people for their services. In 1773 Dr A. Johnson suggested the formation of a similar society in England, and Dr Thomas Cogan translated the memoirs of the Amsterdam society. Dr William Hawes secured a copy and tried to form a society. There was, however, a strong prejudice against the idea, but he publicly offered rewards to persons who, between Westminster and London Bridges, should rescue drowning persons and bring them to certain places on shore in order that resuscitation might be attempted. In this way he was instrumental in the saving of several lives, and paid the rewards out of his own pocket, until his zeal brought him sympathy and the Royal Humane Society was founded. This was in 1774. The system then in vogue was a means of inducing artificial respiration by inserting the pipe of a pair of bellows into one nostril and closing the other. Air was forced into the lungs and then expelled by pressing the chest, thus imitating respiration. Dr Hawes used for his resuscitation work a kind of cradle, in which the subject was placed, and then raised over a furnace. Bleeding, holding up by the heels, rolling on casks, &c. were at various times resorted to. Simple means are often as effective as the official ones. In 1891 a subject was restored in Australia by being held over a smoky fire, which is the native method of restoring life; while a few years back, at an English riverside town, a patient was saved by the placing of a handkerchief over his mouth and the alternate blowing into and drawing air out of the lungs until natural breathing was restored.
One of the oldest methods of resuscitation was that of Dr Marshall Hall (1790-1857), introduced in 1856. In this method the operator takes his place at the patient’s left side, and places a roll of clothing or pillow (which must be the same length as that used in the previous methods), so that it may be in position under the chest when the patient is turned over. The assistant at the head pays particular attention to the patient’s arms, that they may not be laid upon or twisted at the wrists, elbows, hands or shoulders. The patient is then turned face downwards, with the body reclining over the pillow, the operator makes a firm pressure with the hand upon the back, between and on the shoulder blades, he then pulls the patient slowly up on to the side towards himself. Once in position, the operator pushes the patient back again until the face is downward, when the pressure on the back is to be repeated. These three movements must be continued at the rate of about fifteen times a minute, until natural breathing has been restored.
Then came the methods of Dr H. R. Silvester and Dr Benjamin Howard, of New York.
When using the Silvester method, or, for the matter of that, any other method, the first thing to do is to send for medical assistance. Dr Silvester recommended that the patient should not be carried face downwards or held up by his feet. All rough usage should be avoided, especially twisting or bending of limbs, and the patient must not be allowed to remain on the back unless the tongue is pulled forward. In the event of respiration not being entirely suspended when a person is lifted out of the water, it may not be necessary to imitate breathing, but natural respiration may be assisted by the application of an irritant substance to the nostrils and tickling the nose. Smelling-salts, pepper and snuff may be used, or hot and cold water alternately dashed on the face or chest. Provided no sign of life can be seen or felt or the heart’s action heard, promotion of breathing, not circulation must be the first aim and effort. Lay the patient flat on his back, with the head at a slightly higher level than the feet. Remove all tight clothing about the neck, chest and abdomen, and loosen the braces, belts or corsets. The operator taking his place at the head, with an assistant on one side, will turn the patient over until he is lying face downwards, his head resting upon one arm. He should then, after the assistant has given one or two sharp blows with the open hand between the shoulder blades, wipe and clear the mouth, throat and nostrils of all matter that may prevent the air from entering the lungs, using a handkerchief for this purpose. This being done, the patient should be turned upon his back, the tongue pulled forward and kept in position by means of a dry cloth, handkerchief or piece of string tied round the jaw. Every care must be taken not to let it fall back into the mouth and thus obstruct the air passages. When this work has been accomplished (it should only last a few seconds) the operator at the head should lift the patient, handling the head and shoulders very carefully, in order that the assistant may place a roll of clothing or pillow under the shoulder blades. The roll being placed in position, the operator will lean forward and grasp the arms below the elbows. He will then draw the patient’s arms steadily upwards and outwards, above the head, until fully extended in line with the body. Having held the arms in this position for about one second, the operator will carry them back again and press them firmly against the side and front of the chest for another second. By these means an exchange of air is produced in the lungs similar to that effected by natural respiration. These movements must be repeated carefully and deliberately about fifteen times a minute, and persevered in. When natural respiration is once established, the operator should cease to imitate the movements of breathing, and proceed with the treatment for the promotion of warmth and circulation.
Friction over the surface of the body must be at once resorted to, using handkerchiefs, flannels, &c., so as to propel the blood along the veins towards the heart, while the operator attends to the mouth, nose and throat. The friction along the legs, arms and body should all be towards the heart and should be continued after the patient has been wrapped in blankets or some dry clothing. As soon as possible, the patient should be removed to the nearest house and further efforts made to promote warmth by the application of hot flannels to the pit of the stomach, and bottles or bladders of hot water, heated bricks, &c. to the armpits, between the thighs and to the soles of the feet. If there be pain or difficulty in breathing, apply a hot linseed meal poultice to the chest. On the restoration of life, a teaspoonful of warm water should be given; and then, if the power of swallowing has returned, very small quantities of wine, warm brandy and water, beef tea or coffee administered, the patient kept in bed, and a disposition to sleep encouraged. The patient should be carefully watched for some time to see that breathing does not fail, and, should any signs of failure appear, artificial respiration should at once be resumed. While the patient is in the house, care should be taken to let the air circulate freely about the room and all overcrowding should be prevented.
In the Howard method there are only two movements; its knowledge is said to be necessary in case the patient’s arm be in any way injured, or a more vigorous method than the “Silvester” deemed necessary, but care should be exercised not to injure the patient by too forcible pressure. The patient is laid on his back, the roll is larger than that used in the Silvester method, and is placed farther under the back in order that the lower part of the chest may be highest. After adjusting the roll, the operator kneels astride of the patient, while his assistant goes to the head, lifts the patient’s arms beyond the head, and holds them to the ground, cleans the mouth and nose, and attends to the tongue. The operator, with his fingers spread well apart, taking care that the thumbs do not press into the pit of the stomach, grasps the most compressible part of the lower ribs, and with both hands applies pressure firmly by leaning over the patient; then he springs back, lifting his hands off the patient. Artificial respiration is thus effected, and continued at the rate of about fifteen times a minute. When natural breathing has been restored, the treatment is the same as in the Silvester method.
These methods have now been superseded by the Schäfer method, which has been taken up by the Royal Life Saving Society, a body instituted in 1891 for the promotion of technical education in life saving and resuscitation of the apparently drowned. The Schäfer method has much to recommend it, owing to its extreme simplicity and the ease with which the physical operations necessary to carry on artificial respiration may be performed, hardly any muscular exertion being required. It involves no risk of injury to the congested liver or to any other organ, and as the patient is laid face downwards, there is no possibility of the air passages being blocked by the falling back of the tongue into the pharynx. The water and mucus can also be expelled much more readily from the air passages through the mouth and nostrils.
It was due to the happy selection of Professor E. A. Schäfer, as chairman of a committee appointed by the Royal Medical & Chirurgical Society for the investigation of the methods in use for resuscitation of the apparently drowned, that the new method was devised. This committee made many experiments upon the cadaver but failed to arrive at any definite conclusion by that means. The necessity then appeared of thorough investigation of the subject by experiments upon animals, so that the phenomena attendant upon drowning might be better known, and the various methods of resuscitation properly tried. These experiments were made in Edinburgh by Professor Schäfer, with the co-operation of Dr P. T. Herring, and the results obtained were embodied in the report of the committee, which was presented to the Royal Medical and Chirurgical Society in 1904, and published as a supplement to volume 86 of the Transactions of the society. As the direct outcome of these experiments, Professor Schäfer was led to believe that a pressure method of resuscitation was not only simpler to perform but also more efficacious than any other. This conclusion was put to the test by measurements of the results obtained upon the normal human subject by the various methods in vogue; from these measurements, which were published in the Proceedings of the Royal Society of Edinburgh in December 1903, it appeared that when such pressure is exerted in the prone position the highest degree of efficiency as well as simplicity is obtained. The description of this method was communicated to the Royal Medical and Chirurgical Society, and was published in the following year (1904) in volume 87 of the Transactions of the society.
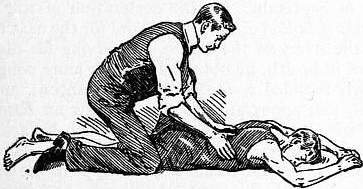 |
| Fig 8..—Schäfer method of treatment of the apparently drowned. Position A. |
Thus it came about that by investigating the phenomena of drowning, and the means of resuscitation in dogs, and by applying the results obtained to man, the method which the society now advocates as the best was arrived at. In the experiments referred to, it was found necessary to drown 38 dogs, all but two of which were from first to last in a complete state of anaesthesia, the two exceptions having been simply drowned without anaesthesia. It is important that the public should understand that the evolution of a method which will probably be the means of saving thousands of lives has resulted from the painless sacrifice of less than 40 dogs, a number which would doubtless in any case have been destroyed by drowning or some other form of suffocation, but without the benefit of the anaesthetics which were employed in the experiments.
 |
| Fig. 9.—Schäfer method of treatment of the apparently drowned. Position B. |
Professor Schäfer describes the method as follows:—Lay the subject face downwards on the ground, then without stopping to remove the clothing the operator should at once place himself in position astride or at one side of the subject, facing his head and kneeling upon one or both knees. He then places his hands flat over the lower part of the back (on the lowest ribs), one on each side (fig. 8), and then gradually throws the weight of his body forward on to them so as to produce firm pressure (fig. 9)—which must not be violent, or upon the patient’s chest. By this means the air, and water if any, are driven out of the patient’s lungs. Immediately thereafter the operator raises his body slowly so as to remove the pressure, but the hands are left in position. This forward and backward movement is repeated every four or five seconds; in other words, the body of the operator is swayed slowly forwards and backwards upon the arms from twelve to fifteen times a minute, and should be continued for at least half an hour, or until the natural respirations are resumed. Whilst one person is carrying out artificial respiration in this way, others may, if there be opportunity, busy themselves with applying hot flannels to the body and limbs, and hot bottles to the feet, but no attempt should be made to remove the wet clothing or to give any restoratives by the mouth until natural breathing has recommenced.
In his paper read before the Royal Society of Edinburgh in December 1903 Professor Schäfer gave the following table of the relative exchanges of air under different methods:—
| Mode of Respiration. | Number per minute. |
Amount of air exchanged per respiration. |
Amount of air exchanged per minute. |
| Natural respiration (supine) | 13 | 489 c.c. | 6.460 c.c. |
| Natural ” (prone) | 12.5 | 422 ” | 5.240 ” |
| Prone (pressure), “Schäfer” | 13 | 520 ” | 6.760 ” |
| Supine (pressure), “Howard” | 13.6 | 295 ” | 4.020 ” |
| Rolling (with pressure), “Marshall Hall” | 13 | 254 ” | 3.300 ” |
| Rolling (without pressure), “Marshall Hall” | 12 | 192 ” | 2.300 ” |
| Traction (with pressure), “Silvester” | 12.8 | 178 ” | 2.280 ” |
These experiments all tend to show that by far the most efficient method of performing artificial respiration is that of intermittent pressure upon the lower ribs with the subject in the prone position or face downward. It is also the easiest to perform, requiring practically no exertion, as the weight of the operator’s body produces the effect, and the swinging forwards and backwards of the body some thirteen times a minute, which alone is required, is by no means fatiguing, and has the further great advantage that it can be effectively carried out by one person.
See Taylor, Medical Jurisprudence; “Description of a simple and efficient method of performing artificial respiration in the human subject, especially in cases of drowning,” by E. A. Schäfer, F.R.S. (vol. 87, Medico-Chirurgical Society’s Transactions); “The relative efficiency of certain methods of performing artificial respiration in man,” by E. A. Schäfer, F.R.S. (vol. 23, part i. Proceedings of the Royal Society of Edinburgh); A Method for the Treatment of the Apparently Drowned, by R. S. Bowles (London, 1903); Handbook of Instruction, Royal Life Saving Society (London, 1908).
Penal Use of Drowning.—As a form of capital punishment, drowning was once common throughout Europe, but it is now only practised in Mahommedan countries and the Far East. Tacitus states that the ancient Germans hanged criminals of any rank, but those of the low classes were drowned beneath hurdles in fens and bogs. The Romans also drowned convicts. The Lex Cornelia ordained that parricides should be sewn in a sack with a dog, cock, viper and ape, and thrown into the sea. The law of ancient Burgundy ordered that an unfaithful wife should be smothered in mud. The Anglo-Saxon punishment for women guilty of theft was drowning. So usual was the penalty in the middle ages that grants of life and death jurisdiction were worded to be “cum fossa et furca” (i.e. “with drowning-pit and gallows”). The owner of Baynard’s Castle, London, in the reign of John, had powers of trying criminals, and his descendants long afterwards claimed the privileges, the most valued of which was the right of drowning in the Thames traitors taken within their jurisdiction. Drowning was the punishment ordained by Richard Cœur de Lion for any soldier of his army who killed a fellow-crusader during the passage to the Holy Land. Drowning was usually reserved for women as being the least brutal form of death-penalty, but occasionally a male criminal was so executed as a matter of favour. Thus in Scotland in 1526 a man convicted of theft and sacrilege was ordered to be drowned “by the queen’s special grace.” In 1611 a man was drowned at Edinburgh for stealing a lamb, and in 1623 eleven gipsy women suffered there. By that date the penalty was obsolete in England. It survived in Scotland till 1685 (the year of the drowning of the Wigtoun martyrs). The last execution by drowning in Switzerland was in 1652, in Austria 1776, in Iceland 1777; while in France during the Revolution the penalty was revived in the terrible Noyades carried out by the terrorist Jean Baptiste Carrier at Nantes. It was abolished in Russia at the beginning of the 18th century.
↧ Download as ZWI file | Last modified: 11/17/2022 15:23:06 | 12 views
☰ Source: https://oldpedia.org/article/britannica11/Drowning_and_Life_Saving | License: Public domain in the USA. Project Gutenberg License
 ZWI signed:
ZWI signed: